


Landmark Petition to Suspend mRNA COVID-19 Shots and Conduct a Full Safety Review officially filed with the FDA
Citizens MAHA—Mobilizing Advocacy to Heal America! has filed a citizen petition positioned to create maximum pressure on the FDA and HHS to remove dangerous mRNA vaccines from the market.

OFFICIALLY SUBMITTED TO THE FDA ON FEB. 13, 2025.
A. ACTION REQUESTED
Pursuant to 21 C.F.R. § 10.30, the undersigned submits this petition under Section 564 of the Federal Food, Drug, and Cosmetic Act (FDCA) and Section 351 of the Public Health Service Act to request that the Secretary of Health and Human Services, the incoming FDA Commissioner upon Senate confirmation, or other designated officials take immediate regulatory action regarding mRNA COVID-19 vaccines. Specifically, the petitioner requests that the FDA:
Immediately suspend all Emergency Use Authorizations (EUAs) and Biologics License Applications (BLAs) for mRNA COVID-19 vaccines, including those manufactured by Pfizer-BioNTech and Moderna, pending a full safety reassessment.
Establish an independent safety review board composed of experts in vaccinology, epidemiology, cardiology, neurology, immunology, and toxicology—free of financial conflicts of interest—to conduct a comprehensive evaluation of mRNA COVID-19 vaccine safety data.
Revoke administrative extensions granted to Pfizer-BioNTech and Moderna for postmarketing safety studies and enforce immediate compliance with outstanding postmarketing requirements related to myocarditis, pediatric safety, and long-term adverse events.
Withdraw EUA and BLA approvals if the independent safety review confirms that mRNA vaccines pose risks that outweigh their benefits or are inconsistent with EUA or BLA standards.
Mandate full disclosure and public release of all validated safety signals and safety data, including findings from VAERS, V-safe, EudraVigilance, and other pharmacovigilance systems, ensuring transparency in regulatory decision-making.
Re-evaluate the FDA-2021-P-0460 petition in light of newly available evidence on mRNA vaccine safety risks and regulatory failures.
Initiate an internal fraud investigation within the HHS, through the Office of Inspector General, to determine whether Pfizer-BioNTech and Moderna engaged in willful misconduct and fraudulent misrepresentation in securing EUA and BLA approvals for their COVID-19 vaccines, and if sufficient evidence of fraud or misconduct is found, formally refer the findings to the Department of Justice for enforcement under the False Claims Act.
The petitioner asserts that continued authorization of mRNA COVID-19 vaccines without immediate suspension poses an unacceptable risk to public health. The requested actions will ensure regulatory transparency, restore public confidence, and prevent further harm.
B. STATEMENT OF GROUNDS
The advent of mRNA vaccines during the COVID-19 pandemic represented a significant shift in modern medicine, deploying a novel and unproven technology at mass scale against a global health crisis. Utilizing lipid nanoparticles (LNPs) to deliver synthetic mRNA encoding the SARS-CoV-2 spike protein, these vaccines were intended to stimulate an immune response. However, emerging evidence reveals substantial risks associated with these vaccines, calling into question their continued use in public health programs. This petition argues unequivocally for the removal of mRNA vaccines from the market based on their systemic harms, biodistribution, persistence, inflammatory properties, and generally unprecedented number and seriousness of adverse events.
Legal Justifications for the Suspension of EUA and BLA Authorizations for mRNA COVID-19 Vaccines
1. Under 21 U.S.C. § 360bbb-3(c), an EUA must be revoked if risks outweigh benefits. Under 21 U.S.C. § 355(e), “Withdrawal of approval; grounds; immediate suspension upon finding imminent hazard to public health,” a BLA must be withdrawn if postmarketing data confirms safety concerns such that the new data demonstrates the drug is unsafe or ineffective under its approved use. The suspension should remain in effect indefinitely, pending a full, independent safety review to determine:
Whether the risks of these vaccines outweigh their benefits for all or certain population groups.
Whether systemic harms identified in postmarket surveillance render the vaccines incompatible with EUA and BLA standards.
2. Emergency Use Authorization (EUA): Section 564 of the Federal Food, Drug, and Cosmetic Act (FDCA) provides the legal framework for the issuance of an Emergency Use Authorization (EUA). This framework requires that:
A. The product addresses a public health emergency.
B. The known and potential benefits outweigh the known and potential risks.
C. No adequate, approved, or available alternatives exist.
The evidence reviewed demonstrates that the mRNA COVID-19 vaccines no longer satisfy these criteria.
3. Public Health Emergency Justification: The declared public health emergency driving the original EUA issuance has shifted with evolving epidemiological trends. Data indicates that SARS-CoV-2 has demonstrably transitioned into endemicity, with declining hospitalization and mortality rates across all demographics, including both vaccinated and unvaccinated populations. As such, the justification for emergency use of a product with substantial safety concerns has evaporated. The FDA has historically revoked EUAs when an emergency no longer warrants their use—failure to do so in this case constitutes a regulatory double standard.
4. Risk-Benefit Imbalance
· Severe Adverse Events: The unprecedented volume of reported adverse events in pharmacovigilance systems, including over 37,000 deaths and millions of other severe reactions, undermines the initial assumption that the benefits outweigh the risks.
· High-Risk Groups: Certain populations, such as young males, face a higher risk of vaccine-related adverse events, including myocarditis and pericarditis, compared to their risk from COVID-19 itself. Studies suggest that the incidence of myocarditis among vaccinated young males is as high as 1 in 3,772, far exceeding safety thresholds historically deemed acceptable for other vaccines. This is a frequency of harm that would have led to immediate withdrawal under prior vaccine safety standards.
· Efficacy Concerns: The emergence of vaccine-evading variants and evidence of rapidly waning immunity undermine the long-term benefits initially anticipated.
5. Availability of Alternatives: FDA-approved therapeutics, including antiviral treatments (e.g., Paxlovid), monoclonal antibodies, traditional protein-based vaccines, explicitly meet the legal definition of 'adequate and available alternatives' under Section 564(c) of the FDCA. This development negates the original "no alternatives" clause justifying the EUA. The continued EUA status of mRNA vaccines is therefore a clear violation of statutory requirements.
6. Biologics Licensure Application (BLA): Section 351 of the Public Health Service Act outlines the stringent criteria for full licensure of biologic products, including:
A. Demonstration of safety and efficacy through rigorous clinical trials.
Consistency in manufacturing processes.
Comprehensive pre-licensure and post-market surveillance.
The mRNA COVID-19 vaccines fall short of meeting these criteria based on the following:
7. Failure to Demonstrate Safety
· Clinical trial data have been critiqued for underreporting adverse events and excluding certain high-risk populations. Subsequent real-world data reveal safety signals, including myocarditis, neurological disorders, and autoimmune conditions, which were not adequately addressed in pre-licensure evaluations.
· Independent analyses of VAERS, EudraVigilance, and similar systems highlight consistent patterns of severe adverse events that exceed historical safety thresholds for licensed vaccines.
8. Manufacturing Inconsistencies: Regulatory agencies, including the European Medicines Agency (EMA) and FDA, have identified batch-to-batch variability and contamination issues. For example, stainless steel contaminants were found in Moderna vaccine vials in Japan, prompting the recall of 1.6 million doses[i] and FDA inspections flagged deviations from Good Manufacturing Practices (GMP), including lack of sterility validation and incomplete quality control documentation.[ii] Such inconsistencies undermine confidence in product safety and efficacy.
9. Inadequate Post-Market Surveillance: Post-market studies have failed to adequately address long-term risks, such as potential carcinogenicity, immune dysregulation, and reproductive impacts. Emerging data on persistent spike protein expression raise concerns about chronic inflammatory conditions and oncogenic pathways.
Such post-market surveillance failures have systematically deprived the public of critical safety data. Under 21 U.S.C. § 355(k), the FDA is legally required to monitor adverse event reports and take corrective action if new risks emerge. The continued authorization of mRNA COVID-19 vaccines despite persistent pharmacovigilance warnings constitutes regulatory negligence and a failure of statutory oversight.
10. Efficacy Concerns and Risk-Benefit Reevaluation: Real-world evidence indicates diminished efficacy against infection and transmission, particularly with new variants. This undermines the initial efficacy claims supporting BLA approval.
11. The COVID-19 pandemic precipitated an unprecedented global response, including the rapid development and deployment of novel mRNA vaccine technologies under EUAs. Unfortunately, mounting evidence now raises substantial concerns regarding their safety, efficacy, and long-term impact on human health. This petition seeks to address these concerns and urges the FDA to act decisively in light of its mandate to protect public health.
12. Findings from peer-reviewed studies, global pharmacovigilance systems, and real-world clinical observational analyses underscore a troubling safety profile associated with mRNA COVID-19 vaccines, including the widespread reporting of severe adverse events such as myocarditis, pericarditis, thrombosis, and neurological conditions. This evidence calls into question whether the known and potential benefits of these vaccines continue to outweigh their known and potential risks, as required under both EUA and BLA frameworks. The petitioner asserts they do not.
13. The FDA has a statutory obligation to ensure the safety, efficacy, and integrity of biologics regulation. The delays in post-marketing safety requirements and incomplete transparency around safety signals present significant concerns that must be addressed to maintain public trust and regulatory confidence. This petition emphasizes the need for the FDA to take immediate action to safeguard public health and restore regulatory integrity.
14. This petition is submitted in good faith on behalf of Citizens MAHA and a growing number of individuals who have suffered mRNA vaccine-related injuries or who are deeply concerned about the safety implications of these vaccines. It is grounded in a robust review of scientific literature, pharmacovigilance data, and legal frameworks that govern the authorization and licensure of biologic products. The petitioner respectfully calls upon the FDA to prioritize transparency, accountability, and safety by addressing the concerns outlined in this document and by implementing the recommended actions detailed below, including the immediate suspension of EUA and BLA licensures for mRNA COVID-19 vaccines.
Overwhelming Evidence of Unprecedented Harm
15. The urgency of this petition arises from mounting evidence that the widespread use of mRNA COVID-19 vaccines has introduced significant risks to public health, underscoring a systemic failure in regulatory oversight.
16. Independent experts, government officials, and international coalitions have highlighted critical safety concerns, including the presence of DNA fragments in vaccine doses, as identified by the Florida State Surgeon General.[1] These fragments, coupled with lipid nanoparticles and SV40 promoter DNA, pose unique risks of DNA integration into the human genome, potentially leading to chromosomal instability, oncogenesis, and heritable genetic changes. The presence of DNA fragments and SV40 promoter sequences violates 21 C.F.R. § 610.18, which mandates that biologics be 'free from extraneous material that could adversely affect the product’s safety.' Despite this, the FDA has failed to mandate comprehensive contamination testing, creating an unprecedented regulatory failure with unacceptable genotoxic consequences.
17. Safety and efficacy concerns raised by the Florida Department of Health include:[2]
The mRNA COVID-19 vaccines present a risk of subclinical[3] and clinical myocarditis[4] and other cardiovascular conditions among otherwise healthy individuals.
The mRNA COVID-19 vaccine may be associated with an increased risk of postural orthostatic tachycardia syndrome (POTS).[5]
The mRNA COVID-19 vaccine may be associated with an increased risk of autoimmune diseases including systemic lupus erythematosus (SLE), rheumatoid arthritis, and psoriasis.[6]
Throughout the pandemic, studies across geographic regions found that the mRNA COVID-19 vaccines are associated with negative effectiveness[7] after four to six months. As efficacy waned, studies showed that COVID-19 vaccinated individuals developed an increased risk[8] for infection.
Elevated levels[9] of mRNA and spike protein from the mRNA COVID-19 vaccine persist[10] among some individuals for an indefinite period, which may carry health risks.[11]
Potential DNA integration from the mRNA COVID-19 vaccines pose unique and elevated risk to human health and to the integrity of the human genome, including the risk that DNA integrated into sperm or egg gametes could be passed onto offspring of mRNA COVID-19 vaccine recipients.[12]
There is unknown risk of potential adverse impacts with each additional dose of the mRNA COVID-19 vaccine; currently individuals may have received five to seven doses (and counting) of this vaccine over a 3-year period.
18. Adding to these concerns, The Hope Accord, signed by an international consortium of physicians and scientists, has called for an immediate suspension of mRNA vaccines and full-scale investigations into their safety. The Hope Accord cites high rates of adverse events, including myocarditis, prolonged inflammation, and potential genetic modification, all supported by laboratory and autopsy studies.[13]
19. These findings align with analyses by Doctors for COVID Ethics, who documented DNA contamination in vaccine batches[14] and highlighted mechanisms of harm[15] that apply not only to COVID-19 vaccines but also to the broader mRNA technology platform.[16] Their evidence shows that systemic risks, such as vascular and organ damage, are inherent to these vaccines, exacerbating the need for precautionary measures.
20. Concerns about the integrity of clinical trials and the transparency of data have further eroded public trust. For example, The Pfizer Papers: Pfizer’s Crimes Against Humanity revealed that Pfizer’s mRNA vaccine clinical trials were deeply flawed, including the premature vaccination of placebo group participants and the withholding of critical safety data. These actions irreversibly compromised the ability to assess long-term safety and efficacy. Regulatory agencies, including the FDA, had knowledge of these irregularities yet failed to intervene, a violation of the agency’s duty under 21 U.S.C. § 355(k) to ensure postmarket surveillance of biologics. Analysis of more than 450,000 pages of internal Pfizer documents uncovered massive harms ignored by the FDA, detailed in The Pfizer Papers. This research revealed 1,233 deaths in the first three months of the vaccine rollout, and a litany of injuries: “industrial-scale blood diseases: blood clots, lung clots, leg clots; thrombotic thrombocytopenia, a clotting disease of the blood vessels; vasculitis, dementias, tremors, Parkinson’s, Alzheimer’s, epilepsies.”[17]
21. These harms are echoed by data from V-safe,[18] a smartphone-based tool created by the CDC.[19] Among 10.1 million registered V-safe users, 7.7 percent reported[20] side effects after mRNA COVID-19 vaccination so serious they were compelled to seek medical care, many more than once (Siri 2023).
22. According to CDC[21] figures[22] analyzed[23] in Toxic Shot: Facing the Dangers of the COVID “Vaccines,” from 2021-2023 the US suffered 600,000 excess deaths not associated with Covid.[24] Furthermore, Bureau of Labor Statistics data reveal that two million Americans became newly disabled[25], with unusual excesses in historically low-risk groups. This surge in disability coincided with mass Covid vaccination, including an unaccountable 59 percent surge in deaths among Americans ages 15-44 in the third quarter of 2021 compared to 2019, and must be subjected to immediate epidemiological investigation under the FDA’s postmarket safety obligations. Crucially Covid contributed only part of this excess mortality: in that quarter the US suffered around 201,000 excess deaths, with Covid officially accounting for 123,000, leaving 78,000 excess deaths[26] — 39 percent of the total — still unexplained.
23. Similar[27] figures[28] from[29] abroad[30] underscore[31] a tragic loss of life among healthy people at minimal serious risk from the virus. Hundreds of peer-reviewed studies have demonstrated[32] the spike protein’s potential for harm[33] independent[34] of the rest of the virus[35] – whether from infection or vaccine exposure –induces direct toxicity including myocarditis, blood clots, neurological injuries, and immune dysfunction. Pfizer’s own pre-market biodistribution studies show that vaccine components leave[36] the injection site[37] in the arm and penetrate[38] every major organ system within hours, where mRNA can linger for weeks,[39] forcing cells to churn out more and more of the toxic spike protein, which can persist[40] for months.[41] There is no way to predict[42] how much spike protein the mRNA injections will produce in any individual, and there is no “off switch.”[43]
24. “Medical ethics demand a balanced approach to every intervention, weighing potential benefits against potential harms. However, in the case of the Covid vaccines, federal agencies have chosen only to proclaim benefits. By surfacing data that bear upon both the positive and negative impacts of the Covid vaccines, and evaluating the pandemic performance of CDC, FDA, and other health agencies, the new administration can restore confidence and integrity in medicine and public health,” writes Harvey Risch, a physician and Professor Emeritus of Epidemiology at Yale School of Public Health and Yale School of Medicine.[19]
25. In pursuit of accountability, a lawsuit filed by the Texas Attorney General against Pfizer accuses the company of misleading the public about vaccine efficacy and engaging in efforts to suppress critical safety information. Pfizer’s widespread representation that its vaccine possessed 95% efficacy against infection was intentionally misleading, the lawsuit alleges. That metric represented a calculation of the so-called “relative risk reduction” for vaccinated individuals in Pfizer’s initial, two-month clinical trial results rather than real-world effectiveness. FDA publications indicate “relative risk reduction” is a misleading statistic that “unduly influence[s]” consumer choice, the Texas AG notes.[44]
26. The Texas AG’s lawsuit further contends that Pfizer’s own clinical trial data failed to demonstrate that its vaccine prevented transmission—contradicting the company’s public claims and coercive marketing tactics: “Pfizer fostered a misleading impression that vaccine protection was durable and withheld from the public information that undermined its claims about the duration of protection. And, despite the fact that its clinical trial failed to measure whether the vaccine protects against transmission, Pfizer embarked on a campaign to intimidate the public into getting the vaccine as a necessary measure to protect their loved ones. In fact, Pfizer’s product failed to live up to the company’s representations. COVID-19 cases increased after widespread vaccine administration, and some areas saw a greater percentage of deaths from COVID-19 among the vaccinated population than the unvaccinated.” [44]
27. Together, these findings present an overwhelmingly clear and compelling case for action. As noted above, the Florida Surgeon General’s recent recommendations against the continued use of mRNA vaccines emphasize the potential for long-term harm and the failure of regulatory agencies to enforce adequate safeguards. His statements highlight prolonged spike protein circulation, increased risks of autoimmune disease, and potential DNA integration as critical areas of concern. The FDA cannot continue to ignore these systemic failures without breaching its statutory duty to protect public health.
28. These risks have also been echoed in international advocacy efforts, such as those by The NORTH Group, which demands independent investigations into the safety and approval processes of mRNA vaccines.[45] Bolstered by a comprehensive “Scientific Summary,” (see Appendix B) here are the three critical issues raised by The NORTH Group:
● COVID-19 vaccines were never tested for their ability to block viral transmission.[46] Hence, medical product regulators, as well as governments and governmental bodies, misled people in order to coerce them into accepting these products.
● COVID-19 vaccines resulted in an unprecedented level of reported side effects,[47] including deaths.[48] Reproducible analyses of public data[49] [50] [51] [52] shows that it was a lottery as to which batch a person received and the side effects that they may have experienced.
● Analyses by multiple, independent scientists evidence variable and excessive levels of residual plasmid DNA in vials of Pfizer and Moderna’s products - this foreign DNA is a by-product of the manufacturing processes and should never have made it into commercial vials.
29. In January 2024, the Global Vaccine Data Network (GVDN) published the largest observational vaccine safety study ever conducted, analyzing 99 million vaccinated individuals worldwide. This multinational study, published in a leading peer-reviewed journal, identified statistically significant increases in severe adverse events associated with the mRNA vaccines, including cardiovascular, hematologic, and neurological disorders. The study examined the incidence of a multitude of adverse events of special interest (AESIs) derived from a denominator of nearly a billion doses of BNT162b2 and MRNA-1273 as well as a 3rd vaccine, likely reflecting a substantial portion of what was captured in the Global Safety Databases of Moderna and Pfizer.
30. The results of GVDN’s observational study were alarming. BNTl62b2 was identified with statistically significant increases in the observed versus expected events for the following AESIs[53]:
Neurological Conditions:
Bell's Palsy
Generalized Seizures
Hematologic Conditions:
Thrombocytopenia
Idiopathic Thrombocytopenia
Pulmonary Embolism
Cerebral Venous Sinus Thrombosis
Splanchnic Vein Thrombosis
Cardiovascular Conditions:
Myocarditis
Pericarditis
31. Similarly, MRNA-1273 was identified with statistically significant increases in the observed versus expected events for the following AESIs:
Neurological Conditions:
Bell's Palsy
Acute Disseminated Encephalomyelitis
Febrile Seizures
Generalized Seizures
Hematologic Conditions:
Thrombocytopenia
Pulmonary Embolism
Splanchnic Vein Thrombosis
Cardiovascular Conditions:
Myocarditis
Pericarditis
32. Furthermore, The National Academies of Sciences, Engineering, and Medicine (NAS) published a comprehensive report in April 2024 titled 'Evidence Review of the Adverse Effects of COVID-19 Vaccination and Intramuscular Vaccine Administration.' This independent evaluation of vaccine safety systematically reviewed adverse events associated with COVID-19 vaccines, with a particular focus on mRNA products by Pfizer-BioNTech and Moderna. The report’s findings provide strong, science-based justification for the immediate suspension of these vaccines' licensure and reinforce the urgent need for regulatory reevaluation.[54]
Key NAS Findings Supporting Petition Assertions
33. Establishment of Causality for Myocarditis: The NAS report conclusively determined that mRNA COVID-19 vaccines can cause myocarditis, a severe and potentially life-threatening inflammation of the heart muscle. This finding aligns with extensive peer-reviewed studies and real-world pharmacovigilance data, underscoring that young males, particularly those under 30, face significantly heightened risks of myocarditis following mRNA vaccination. This finding contradicts the original safety assurances provided by manufacturers and regulators, highlighting a serious regulatory failure in accurately assessing the risks for critical subpopulations.
34. Insufficient Evidence to Refute Numerous Safety Concerns: The NAS report found insufficient evidence to rule out a causal relationship for 65 separate adverse events linked to COVID-19 vaccination. This finding underscores severe gaps in regulatory oversight and confirms that safety assessments remain incomplete. The widespread lack of definitive safety data supports this petition’s contention that both pre-market clinical trials and post-market surveillance have failed to adequately evaluate the long-term risks of these vaccines.
35. Insights into Shoulder Injury and Vaccine Administration: The report also identified causal relationships between intramuscular administration and specific shoulder injuries, further illustrating the potential for adverse effects directly linked to the methods of vaccine delivery. While this finding is not exclusive to mRNA vaccines, it reinforces the broader concerns about inadequate consideration of risks in the rushed deployment of these novel products.
36. Importance of Transparent and Rigorous Safety Assessment: The NAS emphasized the importance of comprehensive, transparent, and evidence-based assessments of vaccine safety to maintain public trust and regulatory credibility. The failure to address critical safety signals through robust post-market analysis undermines these goals and reinforces the petition’s call for immediate regulatory action.
Implications for FDA Licensure Withdrawal
37. The NAS report constitutes a definitive independent safety evaluation, exposing fundamental flaws in the regulatory approval process for mRNA vaccines. Its confirmation of myocarditis causality and widespread safety data gaps undermines the foundational risk-benefit calculus used to justify the EUA and BLA. These findings invalidate the premise that the benefits of these vaccines outweigh their risks, warranting immediate regulatory intervention:
The causal link to myocarditis fundamentally contradicts the principle that vaccine benefits must outweigh risks across all populations, particularly when alternative COVID-19 prevention measures now exist.
The insufficient evidence for 65 adverse events reveals systemic flaws in pharmacovigilance and raises legitimate concerns about the lack of comprehensive safety evaluation for these products.
The unprecedented scope of adverse events identified in real-world data, combined with the NAS findings, demands an urgent reassessment of the risk-benefit calculus underpinning the Emergency Use Authorization (EUA) and Biologics Licensure Application (BLA) approvals.
38. An analysis by the Association of American Physicians and Surgeons (2024) of Medicare mortality data reveals a statistically significant increase in death rates following COVID-19 vaccination. This alarming trend has been observed consistently across multiple nations, ruling out geographical anomalies and reinforcing concerns of a causal relationship between mRNA vaccination and excess mortality. These findings demand immediate federal investigation and reinforce the necessity of halting further administration of these vaccines.[55]
39. The observed increase in post-vaccination death rates challenges the presumption that COVID vaccines deliver a clear net benefit, especially in populations that do not face high risks from COVID-19 itself. This supports the petition's argument about the failure of the risk-benefit balance for certain key demographics. From the AAPS report:
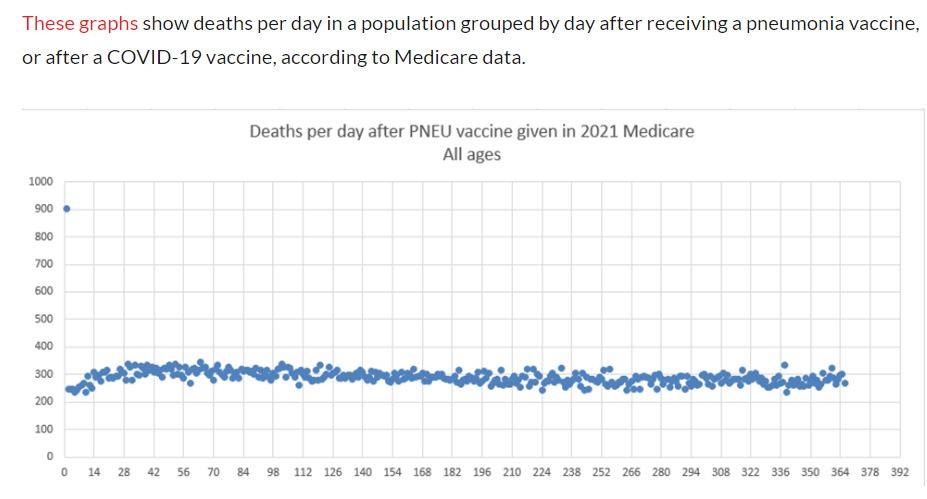
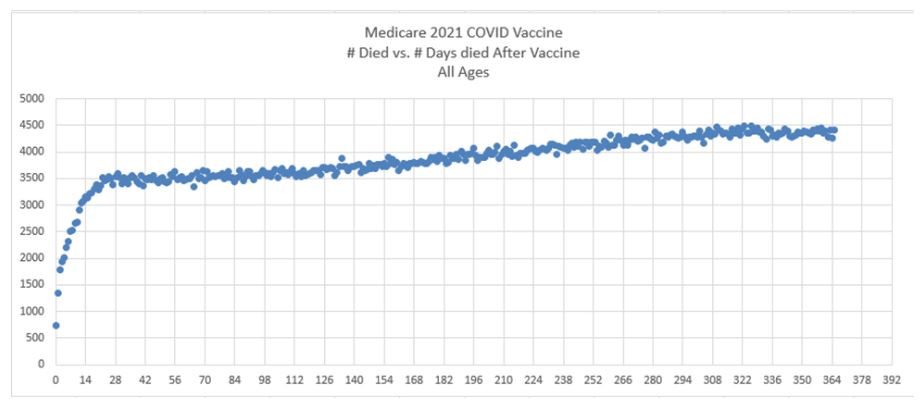
40. “For a safe vaccine, the line always slopes downward after a brief upward slope for the death rate to get to baseline. (There should be fewer early deaths in this cohort because of the temporary healthy vaccinee effect. This effect lasts up to 21 days or so.) People only die once, so there are fewer people left in the cohort to die as time passes,” the AAPS report finds. The upward slope for the COVID vaccine is unique, according to this analysis. After the first shot, an average 3492 deaths per day increased to 4365 deaths per day, an increase of 25% over one year. There is no background event to account for this and the same effect is seen in every country for which the author has data. This data appears to be an incontrovertible smoking gun exposing the danger of the mRNA COVID-19 vaccine platform and the lack of safety involved with these vaccines.
Vaccine-Related Myocarditis and Pericarditis (VRMP)
41. The scientific and medical communities have been engaged in a four-year debate about how common VRMP events truly are. According to the Final Report of the Florida Grand Jury Report (2024) investigating potential criminal activity by mRNA COVID-19 vaccine manufacturers, which surveyed this topic, one of Pfizer's representatives provided to the Grand Jury the low VRMP rate estimate of ten cases per 1 million vaccinated, or one per 100,000.[56] However, the report notes, at the other end of the spectrum, a much higher estimate of 373.2 per million, or one case of VRMP per 2,680 vaccinated individuals who received their second dose of BNT162b, was found in a study of Hong Kong adolescents. This population-based cohort study may highlight Hong Kong’s robust pharmacovigilance system, capturing real-world data on adverse events with greater sensitivity than systems in many other countries.
42. As the Grand Jury Report notes, it is “important to keep in mind that death is not the only negative outcome that can arise from VRMP. All myocarditis and pericarditis events can lead to long-term damage and scarring of the cardiac muscle. This scarring can permanently compromise the heart's performance, potentially causing serious problems later in life. The danger posed by these negative outcomes means that diagnoses of VRMP have a hospitalization rate approaching 100%. In short, the FDA classifies myocarditis and pericarditis as SAEs [Serious Adverse Events] for a reason.” According to an authoritative study of myocarditis and pericarditis in healthy military servicemembers from 2002-03, the baseline population rate of myocarditis is roughly 21.6 per million, or one per 46,300. Numerous studies of VRMP have found the rate to be orders of magnitude greater than the baseline population rate.
43. Importantly, the Grand Jury Report notes, studies of VMRP that include appropriate statistical steps towards stratification (separately analyzing men under the age of 40, for example) tend to find higher rates of VRMP in the highest-risk groups, yielding less favorable risk-benefit ratios for vaccine administration in those groups. On the other hand, the failure to adequately stratify that occurs in many VRMP analyses tends to cause higher risk groups to be lumped in with lower risk groups, making risks appear lower in those at highest risk and ultimately biasing their conclusions. This phenomenon is described in COVID-19 vaccine induced myocarditis in young males: A systematic review, published in January of 2023.[57]
44. For the purposes of conducting accurate risk-benefit analysis regarding the safety profile of mRNA COVID-19 vaccines, it is imperative to ascertain an accurate understanding of the true risk of VRMP, yet existing studies are widely disparate and based on differing methodologies, reporting systems and populations. After undertaking a thorough review of the evidence, the Florida Grand Jury concluded that a 2022 Nordic cohort study of 23 million residents “is probably the most reliable overall result.” In this study, VRMP risk in all age groups is elevated at least slightly with second doses of both MRNA-1273 and BNT162b2, but the risk is more pronounced for MRNA-1273 with 77.4 excess events per million per second dose. However, in the more limited demographic of males aged 16 to 24-years-old,, the number was much higher, with BNT162b2 being estimated to cause 83.0 excess events per million per second dose and MRNA-1273 being estimated to cause an alarming 265.1 excess events per million per second dose (1 per 3772 doses).[58]
45. The criteria employed for what evidence qualifies as a "case" of myocarditis are defined by the Brighton Collaboration, a non-profit global vaccine safety research network, and they are known as the Brighton Collaboration Criteria (BCC). While I will not repeat the Florida Grand Jury’s investigative process in full in this petition, it is crucial to consider in depth by the reviewers of this petition because “this Grand Jury, through its subpoena process, was able to obtain a vast number of pharmacovigilance reports involving potential SAEs of VRMP that were submitted to Pfizer and Moderna from sources around the world.”
46. The Florida Grand Jury’s finding on page 94 of their final report is extremely salient: “Based on the testimony of its own representative and its own records, Modema's approach to myocarditis classification-especially in cases involving alternative etiologies-is clearly at odds with the BCC. Not only does this apparently result in fewer SAEs of "myocarditis," the logic also conveniently excludes any reported cases of myocarditis that involve other cardiac complications, resulting in a less severe characterization of VRMP overall. Any potential complication appears to be used as a means for excluding the case altogether, rather than standing as a data point that VRMP may sometimes present with serious cardiac complications.” If true as charged, this is compelling evidence of dishonest pharmacovigilance that throws into doubt the entire basis for the approval and licensure of the vaccine.
47. The above finding alone provides a strong justification for the suspension of licensure for the Moderna COVID-19 vaccine pending comprehensive safety review, and it is compounded by other sources of evidence. Prioritization of safety now demands the suspension, safety review and withdrawal of licensure for these vaccines by the FDA.
Overview of Studies Highlighting Elevated Myocarditis/Pericarditis Risks
48. Numerous Multiple large-scale international studies confirm that the real-world incidence of myocarditis following mRNA vaccination far surpasses the 1 in 100,000 rate claimed by Pfizer representatives. These studies, conducted in Ontario, Israel, the United States, the Nordic countries, and the military, consistently show that young males face dramatically elevated risks, particularly following second doses of mRNA vaccines. This evidence demands an urgent reevaluation of the safety profile of mRNA vaccines and immediate regulatory intervention to prevent further harm:
A. Ontario Population-Based Study (Buchan et al., 2022)[59]
· Found rates of myocarditis/pericarditis following a second dose of mRNA-1273 (Moderna) as high as 299.5 cases per million in males aged 18–24 years.
· The study also reported elevated rates for BNT162b2 (Pfizer), with rates up to 97.3 cases per million in males aged 12–17 years.
B. Israeli Surveillance Study (Mevorach et al., 2021)[60]
· Documented myocarditis rates of 150 cases per million second doses in males aged 16–19 years during periods of both passive and active surveillance.
C. US Vaccine Safety Datalink Analysis (Shimabukuro 2022)[61]
· Confirmed myocarditis/pericarditis rate of 65.7 cases per million second doses of mRNA-1273 in males aged 18–25 years within zero to 7 day risk interval; excess cases of 61.8 per million.
D. Nordic Cohort Study (Karlstad et al., 2022)[58]
· Found rates of myocarditis following mRNA-1273 vaccination to be 2.6 times higher than for BNT162b2 in males aged 16–24 years.
· 40 to 70 excess events within 28 days per 1 million vaccinees after a second dose of BNT162b2, and 90 to 280 excess events within 28 days per 100 000 vaccinees after a second dose of mRNA-1273.
· Rates ranged from 56 to 184 per million doses, depending on age and dose number.
E. US Military Study (Montgomery et al., 2021)[62]
· Identified a rate of 19.8 cases per million doses among male military personnel, noting an underreporting tendency in younger, healthy populations.
49. Key Insights Across Studies: The findings of these studies underscore the urgent need to reassess the safety profile of mRNA COVID-19 vaccines, particularly in populations at elevated risk. The higher-than-expected incidence rates of myocarditis and pericarditis challenge the initial assumptions underpinning the EUA and BLA approvals and demand immediate regulatory action.
Consistent identification of higher risks among young males, particularly after the second dose.
Variation in reported rates due to differences in surveillance methodologies, intervals between doses, and population demographics.
Real-world evidence suggests that the true risk of myocarditis and pericarditis following mRNA vaccination may exceed previously reported estimates.
50. This evidence also highlights systemic gaps in postmarket surveillance and the importance of implementing robust pharmacovigilance measures to identify and address safety risks promptly. The failure to disclose and transparently investigate safety signals undermines public trust and contradicts the FDA’s commitment to safeguarding public health.
[Note: References before this point are listed in the endnotes. References for the next section are contained in Appendix A.
A subsequent note will be provided upon resumption of endnote references.]
51. The following section examines the systemic harms associated with mRNA COVID-19 vaccines, focusing on biodistribution, persistence, inflammatory properties, and their broader physiological implications. Contrary to early claims that mRNA vaccines remain localized at the injection site, emerging evidence demonstrates widespread dissemination and prolonged presence of vaccine components in critical organs, raising serious safety concerns.
52. One of the most alarming concerns is the biodistribution of mRNA and spike protein. Traditional vaccines are designed to remain localized at the injection site, where immune activation occurs primarily in regional lymph nodes. However, mRNA vaccines, encapsulated in lipid nanoparticles (LNPs), demonstrate a markedly different biodistribution pattern. Studies have confirmed that vaccine-derived mRNA and spike protein reach vital organs—including the heart, liver, brain, lungs, spleen, and reproductive tissues such as the ovaries and testes—where their presence correlates with inflammatory and immune-mediated pathologies. The spike protein’s ability to cross critical physiological barriers, such as the blood-brain barrier, further exacerbates these risks. For instance, studies have linked spike protein infiltration into the brain with inflammation and encephalitis, while its presence in cardiac tissue correlates with myocarditis and arrhythmic dysfunction. Such findings underscore the systemic and unintended consequences of these vaccines.
53. Equally troubling as a major unresolved safety concern is the prolonged persistence of both vaccine mRNA and its encoded spike protein in human tissues. Despite early claims that these components would degrade within days, scientific evidence contradicts this assumption. Studies reveal that vaccine-derived mRNA can persist for weeks, while spike protein has been detected in tissues and circulation for up to six months post-vaccination. This persistent presence is unprecedented compared to natural viral infections, in which viral proteins are typically cleared within weeks. The implications of extended exposure to spike protein include prolonged immune activation, chronic inflammation, and potential autoimmune dysregulation. Furthermore, the detection of spike protein in the absence of viral RNA suggests ongoing exposure to a potentially harmful antigen without resolution, a phenomenon not typically observed in natural infections.
54. The lipid nanoparticle (LNP) delivery system introduces additional safety concerns, as it is inherently pro-inflammatory. LNPs protect fragile mRNA from degradation, but their ionizable lipid components activate the immune system in unintended ways. Studies show that LNPs trigger robust inflammatory cascades, notably through interleukin-1β (IL-1β), a potent driver of systemic inflammation. This inflammation has been implicated in autoimmune reactions, cardiovascular dysfunction, and hypersensitivity reactions, including anaphylaxis associated with polyethylene glycol (PEG), a component of the LNPs. Alarmingly, the rate of anaphylaxis associated with mRNA vaccines is markedly higher than that of other vaccines. These findings demand greater scrutiny of the excipients used in mRNA formulations. Additionally, the pro-inflammatory nature of LNPs may exacerbate pre-existing inflammatory conditions, further complicating their safety profile and raising questions about their suitability for widespread use.
55. Mechanistically, the harms associated with mRNA vaccines arise from several interconnected pathways. The spike protein itself exhibits toxic properties, inducing endothelial dysfunction, impairing mitochondrial function, and disrupting critical physiological systems such as the renin-angiotensin system. Its interaction with vascular endothelial cells can lead to inflammation, clot formation, and tissue damage. Moreover, the prolonged presence of spike protein may result in antigenic imprinting, altering immune system memory and potentially reducing the efficacy of future responses to viral variants. Combined with the systemic inflammatory effects of LNPs, these mechanisms create a scenario where immune activation leads to adverse outcomes ranging from mild inflammation to severe, life-threatening conditions.
56. Evidence of systemic harms extends beyond individual cases to broader epidemiological trends. Studies have identified a disproportionately high incidence of myocarditis, pericarditis, and thrombotic events following mRNA vaccination. These findings are consistent across demographic groups, including young, healthy individuals who are at low risk for severe COVID-19. The adverse events reported are not rare anomalies but part of a growing pattern that underscores the inherent risks of this vaccine platform.
57. Moreover, the lack of transparency in addressing these safety concerns has eroded public trust. Initial claims about the safety and efficacy of mRNA vaccines have been contradicted by subsequent research, highlighting the need for rigorous, independent investigations. Regulatory bodies must prioritize public health over pharmaceutical interests by reevaluating the risk-benefit profile of these vaccines. The continued deployment of mRNA vaccines without addressing their systemic harms undermines the integrity of public health initiatives.
58. The overwhelming evidence of widespread biodistribution, prolonged persistence, and inflammatory toxicity warrants the immediate suspension of mRNA COVID-19 vaccines. Regulatory bodies must acknowledge that these vaccines no longer meet the safety standards required for continued licensure. Given the serious risks, including cardiovascular inflammation, immune dysregulation, and persistent spike protein exposure, withdrawing these vaccines is not only justified but necessary to uphold public health protections. Safer alternatives exist, and resources should be redirected toward developing and deploying therapeutics with more favorable safety profiles. Enhanced pharmacovigilance, post-marketing surveillance, and transparent communication are essential to restoring public confidence and ensuring that future vaccination efforts prioritize safety and efficacy. As the scientific community continues to unravel the complexities of these vaccines, the precautionary principle must guide decision-making. Protecting public health requires a proactive approach to mitigating harm, and the withdrawal of mRNA COVID-19 vaccines is a necessary step toward achieving this goal.
We will now explore the issues raised in this section in greater depth with citations.
Extended Persistence of mRNA and Spike Proteins
59. Persistence of mRNA and spike protein antigens associated with mRNA COVID-19 vaccines has raised significant concerns regarding their safety and potential for long-term adverse effects. Multiple peer-reviewed studies confirm that vaccine-derived mRNA and spike protein persist in human tissues for months, contradicting regulatory claims of rapid degradation and raising urgent concerns about long-term toxicity and immune system disruption. For instance, Röltgen et al. (2022) found that vaccine mRNA and spike antigens persisted in germinal centers up to eight weeks post-vaccination, while Brogna et al. (2023) detected spike protein in blood samples as late as 187 days post-vaccination. These findings expose a fundamental failure in regulatory oversight, as the prolonged persistence of vaccine mRNA and spike protein introduces unpredictable long-term risks that were never rigorously evaluated before mass distribution.
60. A growing body of evidence reveals that vaccine mRNA can be detected in various organs and tissues long after administration. Studies such as Boros et al. (2024) report the persistence of mRNA in cardiac and skeletal muscle up to a month post-vaccination, with recombinant spike protein detected for over six months in the bloodstream. Similarly, Castruita et al. (2023) demonstrated the circulation of vaccine mRNA sequences in blood up to 28 days post-vaccination, while Fertig et al. (2022) found mRNA in the bloodstream 15 days post-injection. Furthermore, Pateev et al. (2024) observed spike antigen lingering in lymph nodes up to 60 days after vaccination, underscoring the systemic dissemination of vaccine components.
61. The persistence of the spike protein, a known pathogenic component of the SARS-CoV-2 virus, raises additional concerns about potential harm. Patterson et al. (2022) detected the S1 protein of the spike antigen in CD16+ monocytes for up to 15 months in individuals with post-acute sequelae of COVID-19 (PASC), suggesting a similar duration of persistence for vaccine-derived spike proteins. Fraser et al. (2024) observed spike protein in lung tissues of patients with post-COVID lung disease two years after initial infection. These studies collectively imply that the prolonged presence of spike protein in critical tissues is now scientifically associated with chronic inflammation, immune hyperactivation, and irreversible tissue damage, necessitating immediate regulatory intervention.
62. Specific case reports further illustrate the adverse outcomes associated with vaccine-induced spike protein persistence. Hano et al. (2023) described a patient who developed persistent skin lesions 100 days post-vaccination, with immunohistochemical staining confirming the presence of spike protein in endothelial cells and eccrine glands. Similarly, Kawano et al. (2022) reported a case of fulminant myocarditis 24 days after vaccination, with positive immumostaining for spike protein in myocardial tissue. These findings suggest that prolonged exposure to spike protein can elicit localized inflammatory responses and systemic immune dysregulation.
63. The systemic effects of persistent spike protein are underscored by findings of circulating spike protein in extracellular vesicles. Craddock et al. (2023) demonstrated that spike proteins linked to extracellular vesicles persisted for over a year in individuals with PASC. This persistence suggests that spike protein can evade degradation pathways, potentially contributing to long-term immune dysregulation and chronic inflammatory states. Swank et al. (2022) further linked persistent circulating spike protein to post-acute COVID-19 sequelae, noting its presence in patients up to 12 months after diagnosis, and determining that “detection of spike in PASC patients months after diagnosis suggests the presence of replicating viral reservoirs.”
64. These findings collectively underscore significant concerns about the persistence of mRNA and spike protein components of COVID-19 vaccines and their potential implications for human health. The long-lasting presence of these elements in tissues and circulation contradicts early safety assurances and suggests a need for ongoing monitoring and rigorous investigation. Given the role of spike protein in triggering inflammatory and immune-mediated responses, the prolonged exposure to vaccine-induced spike proteins may exacerbate chronic inflammatory conditions and pose risks for individuals with preexisting vulnerabilities. The breadth and depth of evidence necessitate a reevaluation of vaccine safety protocols and long-term surveillance to mitigate potential harms and better understand the full spectrum of vaccine-induced effects.
Biodistribution and Organ Involvement
65. Pharmacokinetic data from biodistribution studies confirm that lipid nanoparticle-encased mRNA does not remain localized at the injection site but instead spreads systemically, accumulating in vital organs such as the spleen, heart, kidneys, brain, ovaries, and testes, raising significant concerns about long-term toxicity and off-target effects.. The European Medicines Agency reported detectable mRNA in the ovaries and testicles nine days post-vaccination (European Medicines Agency).” Synthetic mRNAs encapsulated in LNPs can reach many organs, such as the spleen, heart, kidneys, lungs and brain,” the EMA Assessment Report found. Such distribution expands the potential for unintended effects beyond the injection site, contradicting the supposed safety profile of these mRNA vaccines.
66. Regulatory agencies must acknowledge that vaccine-induced spike protein has been found in multiple critical organs, where its cytotoxic and inflammatory properties pose severe risks of irreversible tissue damage, including myocarditis, neuroinflammation, and endothelial dysfunction. For example, Karaba et al. (2024) detected spike antigen in plasma two weeks after vaccination in kidney transplant recipients, while Krauson et al.(2024) found it in the axillary lymph nodes and myocardium of patients who died within 30 days of vaccination. “Detectable plasma severe acute respiratory syndrome coronavirus 2 spike antigen is associated with poor antibody response following third messenger RNA vaccination in kidney transplant recipients,” concluded Karaba et al. These findings underscore links to cardiac and systemic adverse events.
67. The sustained presence of vaccine-induced spike protein in the bloodstream and organs is not merely a benign phenomenon but is strongly correlated with a spectrum of severe adverse events, including life-threatening myocarditis, blood clot formation, and persistent inflammatory syndromes. Spike protein has been implicated in vascular inflammation, as demonstrated by Hano et al. (2023), who reported persistent lesions in vascular endothelial cells 100 days after vaccination. Similarly, Yonker et al. (2021) linked spike protein to multisystem inflammatory syndrome in children (MIS-C), persisting for months and contributing to systemic inflammation.
68. Persistent mRNA and spike protein presence may drive chronic inflammation, with implications for tissue damage and fibrosis. Boros et al. (2024) identified inflammatory and fibrotic changes in cardiac and skeletal muscle where mRNA was detected, finding that “clinical studies now report that modified SARS-CoV-2 mRNA routinely persist up to a month from injection and can be detected in cardiac and skeletal muscle at sites of inflammation and fibrosis, while the recombinant spike protein may persist a little over half a year in blood.” Mayordomo-Colunga et al. (2022) and Yamamoto et al.(2022) reported persistent spike protein in intestinal cells and skin lesions, linking it to localized inflammation and necrotizing conditions.
Lipid Nanoparticle Toxicity and Widespread Biodistribution
69. The mRNA COVID-19 injections rely on lipid nanoparticles (LNPs) bonded with
polyethylene glycol (PEG) to deliver mRNA coding for the spike protein antigen into human
cells. However, a growing body of evidence suggests that the ionizable LNPs used in the mRNA injections are highly inflammatory on their own, while PEG has long been recognized as an allergen with the potential to trigger anaphylaxis (a severe, possibly life-threatening allergic reaction). Some research suggests a far higher incidence of anaphylaxis due to the mRNA injections than claimed in official estimates, ranging from 1/2,280 doses (Warren CM et al.) to 1/4,049 (Blumenthal KG et al.) and 1/13,882 (Somiya A et al.). In individuals with pre-existing anti-PEG antibodies, exposure to PEGylated nanoparticles can exacerbate immune responses, increasing the risk of severe reactions (Ju et al., 2022; Klimek et al., 2021). PEG hypersensitivity is further complicated by cross-reactivity with polysorbates, leading to potential allergic responses even in individuals without direct PEG exposure (Stone et al., 2019).
70. Studies have demonstrated that LNPs are highly inflammatory, with ionizable lipids triggering robust immune activation. For instance, Ndeupen et al. (2021) found that, “Intradermal injection of these LNPs alone or in combination with non-coding poly-cytosine mRNA led to rapid and robust innate inflammatory responses, characterized by neutrophil infiltration, activation of diverse inflammatory pathways, and production of various inflammatory cytokines and chemokines.” Korzun et al. (2024) linked LNP-induced inflammation to Toll-like receptor 4 (TLR4) activation, triggering distinct physiologically meaningful responses including “reactogenic signal initiation, pro-inflammatory gene expression, and … robust metrics of sickness behavior in mice.” Beyond inflammation, Gao et al. (2025) reported that LNPs compromise protein stability and cellular proteostasis, subtly inducing cytotoxic stress even without overt damage to cell viability.
71. In addition to acute allergic responses, LNPs have been implicated in broader immuno-toxicological effects. Studies suggest that PEG and other lipid components may interfere with immune homeostasis, leading to altered adaptive immune responses, immune suppression, or immune hyperactivation (Qin et al., 2022; Bitounis et al., 2024). Inflammatory pathways initiated by LNPs have been linked to the exacerbation of pre-existing inflammation, suggesting that individuals with inflammatory conditions may experience heightened adverse reactions (Parhiz et al., 2022). Additionally, biodistribution studies indicate that LNPs do not remain localized at the injection site but instead distribute widely across various organs, including the liver, spleen, and ovaries, raising concerns about off-target effects (Tinari, 2021; Maugeri et al., 2019). Evidence also suggests that systemic circulation of LNPs may lead to endothelial damage,
72. The potential for LNPs to induce genotoxic effects and compromise the endothelial barrier has also been proposed, linking their toxicity to broader cardiovascular and autoimmune concerns (du Preez et al., 2024; Tsilingiris et al., 2022). Furthermore, research suggests that PEGylated nanoparticles can induce accelerated blood clearance (ABC) effects, reducing vaccine efficacy and increasing the likelihood of repeated immune activation upon subsequent exposures (Kozma et al., 2020).
73.Meanwhile, PEG is increasingly implicated in hypersensitivity reactions, including anaphylaxis. PEG-specific antibodies, particularly IgE and IgG, have been identified as key mediators of allergic reactions to the vaccines (Chen et al., 2021; Zhou et al., 2021). The immunogenicity of PEG has been documented in both clinical and preclinical settings, with evidence suggesting that repeated exposure amplifies hypersensitivity risks (Ju et al., 2022; Mouri et al., 2022).
74. Notably, differential immune responses to LNPs have been observed based on sex, with women experiencing higher rates of anaphylaxis and other hypersensitivity reactions (Somiya et al., 2021). This has been attributed to increased prior baseline exposure to PEG-containing products such as cosmetics and pharmaceuticals. Moreover, PEG antibodies have been found to increase following mRNA vaccination, raising concerns about potential cumulative sensitization in the population (Carreno et al., 2022; Yang et al., 2024). Investigations into alternative lipid formulations with reduced immunogenicity are ongoing, but current findings indicate a pressing need for better risk stratification and post-market surveillance of LNP-related adverse events (Bitounis et al., 2024; Wang et al., 2024).
75. Taken together, these findings suggest that the immunological and toxicological profiles of LNPs warrant further scrutiny. The heightened inflammatory responses, hypersensitivity risks, biodistribution patterns, and potential long-term effects necessitate ongoing investigation into safer lipid formulations and improved risk mitigation strategies for susceptible populations. Addressing these safety concerns is critical for minimizing adverse outcomes. Suspension of licensure for mRNA COVID-19 vaccines while independent investigators carry out a comprehensive safety review is the prudent course of action.
76 According to the European Medicines Agency (2020), biodistribution studies revealed the presence of mRNA in several organs, including the spleen, heart, kidneys, lungs, ovaries, and testicles. This widespread distribution raises concerns about off-target effects and unintended interactions within critical tissues. For instance, Mörz (2022) reported cases of multifocal necrotizing encephalitis and myocarditis linked to vaccine-induced spike protein in the brain and heart, highlighting the potential for severe neurological and cardiovascular outcomes.
77. The activation of the complement system—a key component of innate immunity—by LNPs and PEG has been implicated in adverse events such as pseudoallergies and accelerated blood clearance. Bakos et al. (2024) identified the dominance of alternative complement pathway activation in response to LNPs, contributing to heightened inflammatory cytokine production. Further, Kozma et al. (2020) described a "vicious cycle" of complement activation and hypersensitivity, underscoring the complex interplay between immune activation and adverse reactions.
Blood-Brain Barrier Disruption and Its Implications
78. Emerging evidence reveals that the mRNA COVID-19 vaccines pose significant risks to the blood-brain barrier (BBB) and, by extension, to overall neurological health. This section synthesizes critical findings from peer-reviewed studies to highlight the mechanisms by which vaccine-induced spike protein production compromises the integrity of the BBB. These findings warrant immediate regulatory action to withdraw these vaccines from the market and initiate a comprehensive reassessment of their safety profiles.
79. The BBB is a specialized structure comprising tightly joined endothelial cells, astrocytes, and pericytes that protect the brain from circulating toxins, pathogens, and immune cells. Disruption of the BBB compromises this defense, allowing harmful substances to enter the brain and trigger neuroinflammation, oxidative stress, and potentially irreversible neurological damage (Suprewicz et al., 2023; Rhea et al., 2021). Given the critical role of the BBB in maintaining central nervous system (CNS) homeostasis, any agent that compromises its integrity should be subject to rigorous scrutiny.
80. Several potential mechanisms of disruption to the blood-brain barrier have been reported in the medical literature:
A. Direct Effects of Spike Protein: Vaccine-induced spike proteins are implicated in BBB disruption through several pathways. Suprewicz et al. (2023) demonstrated that the spike protein increases BBB permeability by damaging tight junctions, such as ZO-1 and claudin-5, while leaving adherens junctions intact. Similarly, DeOre et al. (2021) identified RhoA activation as a key mechanism by which the spike protein compromises endothelial integrity, leading to enhanced paracellular permeability.
B. Adsorptive Transcytosis: Rhea et al. (2021) documented that the spike protein crosses the BBB via adsorptive transcytosis. This process involves electrostatic interactions between the positively charged spike protein and negatively charged endothelial cells, facilitating spike protein entry into the CNS.
C. Cytokine Storms and Secondary Effects: Vaccine-induced spike proteins can trigger systemic inflammation and cytokine storms, releasing pro-inflammatory mediators such as IL-1β, IL-6, and TNF-α. These cytokines degrade tight junction proteins and increase vascular permeability (Suprewicz et al., 2023; DeOre et al., 2021).
D. Trojan Horse Mechanism: Petrovszki et al. (2022) highlighted the "Trojan horse" mechanism, wherein immune cells carrying spike proteins traverse the BBB, introducing the spike protein and inflammatory mediators into the CNS. This exacerbates neuroinflammation and endothelial damage.
81. The consequences of BBB disruption by vaccine-induced spike proteins are profound. Studies reveal a spectrum of adverse effects, including neuroinflammation, encephalopathy, and increased risk of stroke. Suprewicz et al. (2023) reported that spike protein-induced BBB dysfunction correlates with cognitive impairments and neurological complications such as ischemic stroke, encephalitis, and acute disseminated encephalomyelitis. Furthermore, long-term exposure to spike proteins in the CNS has been associated with neurodegenerative processes.
82. Burkhardt (2022) identified the presence of spike proteins in various organs, including the brain, in post-mortem analyses of vaccinated individuals, underscoring the ability of spike proteins to penetrate the BBB. Buzhdygan et al. (2020) used in vitro models to confirm that the spike protein disrupts BBB integrity, with functional consequences observable in microfluidic systems mimicking human physiology.
Systemic Inflammatory Responses and Long-term Implications
83. mRNA vaccines induce systemic inflammatory responses, largely mediated by the IL-1 family of cytokines. Tahtinen et al. (2022) highlighted how IL-1β release drives a cascade of pro-inflammatory signals, exacerbating reactogenicity and limiting vaccine tolerability. Chronic inflammatory responses have been proposed as mechanisms underlying endothelial dysfunction and glycocalyx degradation, potentially contributing to broader cardiovascular and autoimmune sequelae (du Preez et al., 2024).
Batch Variability and Manufacturing Concerns
84. The variability in LNP composition across vaccine batches adds another layer of concern. Studies by Igyarto and Qin revealed that lot-specific differences in mRNA:LNP ratios correlate with disparate levels of adverse events (Igyarto BZ and Zhen Qin, 2024). These findings underscore the importance of stringent manufacturing quality control to minimize risk. The apparent failure by regulatory agencies to enforce “Good Manufacturing Practices” for these mRNA vaccines calls into question whether batch variability is an inherent problem with this type of pharmaceutical platform or the result of corporate and governmental negligence.
Adverse Effects on Immune Fitness
85. Repeated exposure to mRNA-LNP formulations appears to alter immune fitness. Qin Z et al. (2022) demonstrated that pre-exposure to LNPs suppresses adaptive immune responses and induces long-term changes in innate immunity. This raises questions about the implications of booster doses and potential cumulative immunological burden.
Clinical Data and Real-World Observations
86. Real-world studies consistently report higher-than-expected rates of anaphylaxis. Blumenthal et al. (2021) observed an incidence rate of 2.47 per 10,000 vaccinations, significantly exceeding initial estimates by public health authorities. Similar findings were reported by Warren et al (2021), who documented allergic reactions in up to 1 in 2,280 doses, emphasizing the need for robust pharmacovigilance.
87. Over 38,000 deaths and 219,000 hospitalizations have been reported in VAERS temporally correlated to COVID-19 vaccination as of 2024. These numbers far surpasses the combined total of reported deaths from all other vaccines administered over the past three decades. The harms associated with mRNA COVID-19 vaccines are manifold, encompassing systemic dissemination, immune dysregulation, and organ-specific toxicities. The persistence of vaccine components, coupled with their potential to disrupt physiological barriers and induce autoimmunity, warrants a thorough reevaluation of vaccine safety protocols. These findings underscore the necessity for transparent, long-term safety studies and a reassessment of the risk-benefit calculus for mRNA vaccine deployment.
[Note: Endnote references now resume.]
Reanalysis of Clinical Trial Data Reveals Increased Risk of Serious Adverse Events Following mRNA COVID-19 Vaccination
88. A study by Fraiman et al. (2022) conducted a secondary analysis of the Phase III randomized clinical trials for the Pfizer-BioNTech (BNT162b2) and Moderna (mRNA-1273) COVID-19 vaccines and found a statistically significant increase in serious adverse events among vaccine recipients compared to placebo groups. The study specifically examined serious adverse events of special interest, as categorized by the Brighton Collaboration, a globally recognized authority on vaccine safety. The findings revealed that both vaccines were associated with a markedly increased risk of these serious adverse events. In the Pfizer trial, vaccinated participants had a 36 percent higher risk of experiencing a serious adverse event, with an excess risk of 18.0 events per 10,000 vaccinated individuals. In the Moderna trial, the vaccine group experienced a six percent higher risk of serious adverse events, though the confidence interval for this finding was wider. When data from both trials were combined, the results indicated a 16 percent increased risk of serious adverse events among mRNA vaccine recipients compared to placebo, with an absolute risk difference of 13.2 per 10,000 vaccinated individuals.[63]
89. When the analysis was limited to serious adverse events of special interest, which include known vaccine-related complications such as coagulation disorders, cardiovascular conditions including myocarditis and pericarditis, acute kidney and liver injuries, acute respiratory distress syndrome, and neurological disorders such as Bell’s Palsy and encephalitis, the risks were even more pronounced. The Pfizer vaccine trial demonstrated a 57 percent increased risk of serious adverse events of special interest, translating to an excess risk of 10.1 per 10,000 vaccinated individuals. The Moderna trial showed a 36 percent increased risk of serious adverse events of special interest, with an excess risk of 15.1 per 10,000 vaccinated individuals. When combining both vaccine trials, the overall excess risk for serious adverse events of special interest was 12.5 per 10,000 vaccinated individuals, with a risk ratio of 1.43, indicating a 43 percent higher likelihood of experiencing a serious adverse event of special interest after receiving an mRNA COVID-19 vaccine.
90. In other words, Fraiman et al. found an excess risk of serious adverse events of special interest at a rate of approximately 1 in 800 to 1 in 1,000 vaccinated individuals. The implications of this finding are significant, as they suggest that the risk of serious adverse events following mRNA vaccination are higher than initially estimated. Perhaps the most troubling finding from Fraiman et al.’s analysis is the harm-benefit comparison, which contradicts the original safety claims made by the FDA and vaccine manufacturers. The study compared the excess risk of serious adverse events of special interest caused by vaccination against the reduction in COVID-19 hospitalizations within the same trials. In the Pfizer trial, the excess risk of serious adverse events of special interest, at 10.1 per 10,000, was over four times higher than the vaccine’s estimated reduction in COVID-19 hospitalizations, which was 2.3 per 10,000. Similarly, in the Moderna trial, the excess risk of serious adverse events of special interest, at 15.1 per 10,000, was more than double the vaccine’s reduction in COVID-19 hospitalizations, which was 6.4 per 10,000. These findings suggest that in the original clinical trial populations, the mRNA vaccines caused more severe harm than they prevented. The authors of the study explicitly called for a formal harm-benefit analysis stratified by age, sex, and risk of serious COVID-19 outcomes, noting that younger individuals, those with prior COVID-19 immunity, and individuals without comorbidities likely face an even worse risk-benefit ratio.
91. The study by Fraiman et al. further contradicts the FDA’s original safety review, which had concluded that serious adverse events were "balanced" between vaccine and placebo groups. The authors suggest that flaws in the FDA’s review process, such as analyzing only the number of individuals who experienced a serious adverse event rather than total events, failing to account for multiple serious adverse events in the same individuals, and using an analysis population with different follow-up windows, may have concealed the true extent of vaccine harm. Additionally, the FDA review included thousands of additional participants with minimal post-vaccination follow-up, further diluting safety signals. These discrepancies highlight the urgent need for transparency regarding vaccine safety data and a public release of all participant-level trial data to allow independent safety analyses.
92. Finally, Fraiman et al. caution that post-market safety monitoring efforts may underestimate the true risks of mRNA vaccination due to limitations in pharmacovigilance systems and underreporting biases. The authors emphasize that similar levels of harm in prior vaccines, such as the 1999 Rotavirus vaccine, which was withdrawn after causing intussusception at a rate of approximately one in 10,000, would have historically warranted immediate regulatory action. Given the widespread administration of mRNA COVID-19 vaccines, the authors urge an immediate reassessment of the safety profile of these products.
93. Fraiman et al.’s analysis provides compelling evidence that the original Phase III clinical trials of mRNA COVID-19 vaccines revealed significant and unacceptable safety risks that were not adequately addressed by regulators prior to emergency use authorization. The documented increase in serious adverse events, particularly those affecting the cardiovascular, coagulation, and neurological systems, challenges the original risk-benefit assumptions that purported to justify mass vaccination campaigns. These findings underscore the urgent need for a transparent, independent, and systematic review of mRNA vaccine safety and further bolster the rationale for an immediate suspension of COVID-19 vaccine authorizations pending a full safety review and harm-benefit reassessment.
Systematic Reviews and Meta-Analysis of Adverse Events Following mRNA COVID-19 Vaccination Support Petition
94. A systematic review and meta-analysis by Kouhpayeh and Ansari (2022) provides critical insight into the comparative safety of different COVID-19 vaccine platforms, revealing that mRNA vaccines carry a significantly higher risk of adverse events compared to other vaccine modalities. This study synthesized data from 19 clinical trials, calculating pooled risk ratios (RR) for total, systemic, and local adverse reactions across various vaccine types, including inactivated, vector-based, DNA, protein subunit, and mRNA vaccines.[64]
95. The findings indicate that mRNA vaccines are associated with the highest risk of total adverse events, with a pooled risk ratio of 2.01 (95% CI: 1.82–2.23), substantially exceeding the risks associated with inactivated vaccines (RR = 1.46) and vector vaccines (RR = 1.65). Systemic adverse reactions, such as fever, headache, and fatigue, were also significantly more common following mRNA vaccination (RR = 1.53, 95% CI: 1.08–2.16), compared to other platforms. The risk of local adverse events, including injection site pain, erythema, and swelling, was strikingly higher for mRNA vaccines (RR = 4.96, 95% CI: 4.02–6.11), surpassing all other vaccine types.
96. The study underscores that while systemic and local adverse reactions are common with all COVID-19 vaccines, mRNA vaccines exhibit an unusually high reactogenicity profile. The researchers highlight that the use of lipid nanoparticles and polyethylene glycol (PEG) in mRNA vaccine formulations may contribute to the elevated risk of adverse events, particularly hypersensitivity reactions. The reported rate of vaccine-induced anaphylaxis was also significantly higher for mRNA vaccines compared to traditional vaccines, raising concerns about safety monitoring and post-market surveillance. Additionally, the analysis found that adverse event risks varied across populations, with younger individuals experiencing higher rates of systemic reactions.
97. Another meta-analysis by Yang et al. (2024) provides a crucial examination of immune-mediated adverse events following COVID-19 vaccination, reinforcing significant concerns about the safety profile of both mRNA and vector-based vaccines. The study systematically reviewed 42 studies and conducted a single-arm meta-analysis to assess the incidence and severity of myocarditis and thrombosis, the two most dangerous vaccine-related adverse events. The findings indicate that myocarditis disproportionately affects mRNA vaccine recipients, occurring in 61% of cases linked to vaccination, compared to only 6% among those receiving vector-based vaccines. Conversely, thrombosis is more strongly associated with vector vaccines, accounting for 91% of cases, while only 9% of thrombosis cases were linked to mRNA vaccines.[65]
98. The study also analyzed vaccine-induced thrombotic thrombocytopenia (VITT), revealing that 66% of affected individuals experienced cerebral venous sinus thrombosis (CVST), while 43% suffered intracranial hemorrhage. The pooled incidence rates for deep vein thrombosis and pulmonary embolism among vaccinated individuals were 13% and 23%, respectively, with an alarming 30% case fatality rate. These findings indicate that while myocarditis is a dominant concern for mRNA vaccines, the risk of life-threatening thrombotic events is notably higher for vector-based vaccines.
99. Importantly, the study found a 67% positivity rate in anti-PF4 antibody tests among individuals with vaccine-induced thrombosis, suggesting an autoimmune mechanism similar to heparin-induced thrombocytopenia. This further substantiates concerns that vaccine components, particularly adenoviral vectors, may trigger severe immune responses leading to clotting disorders. Additionally, autopsy studies have linked vaccination to sudden cardiac death and pulmonary embolism, reinforcing the need for rigorous post-market surveillance.
100. While the authors acknowledge that most adverse reactions to COVID-19 vaccines are self-limiting, the high incidence of myocarditis and thrombosis demands greater scrutiny, particularly given the elevated fatality rate associated with vaccine-induced thrombotic events. These findings support the petition’s call for a thorough reassessment of mRNA and vector-based vaccine safety, long-term monitoring of vaccine recipients, and more informed consent regarding the risks of myocarditis, thrombosis, and other serious immune-mediated reactions. The study underscores the urgency of reevaluating current vaccine policies and ensuring that individuals receive transparent information about potential life-threatening risks before vaccination.
101. Furthermore, a systematic review by Yasmin et al. (2023) provides a comprehensive evaluation of cardiovascular complications, thrombosis, and thrombocytopenia following COVID-19 mRNA vaccination, offering critical data that supports the petition to suspend mRNA COVID-19 vaccines. This review analyzed 81 studies encompassing 17,636 individuals who suffered cardiovascular events after receiving an mRNA vaccine. Alarmingly, thrombosis was the most frequently reported adverse event, accounting for 13,936 cases, followed by stroke (758 cases), myocarditis (511 cases), myocardial infarction (377 cases), pulmonary embolism (301 cases), and arrhythmia (254 cases). The overwhelming prevalence of thrombotic events, particularly with the BNT162b2 (Pfizer-BioNTech) vaccine, suggests an urgent need for reconsideration of the risk-benefit profile of these vaccines.[66]
102. Myocarditis, a condition previously downplayed in public health discussions, was a prominent adverse event in this study. The authors note that myocarditis cases were predominantly associated with mRNA vaccination, in line with multiple reports from the Vaccine Adverse Event Reporting System (VAERS) and international health agencies. The study also details the potential immunological mechanisms through which mRNA vaccines may trigger myocarditis, including activation of inflammatory cascades and immune-mediated injury. Given the increasing acknowledgment of post-vaccination myocarditis among younger males, these findings call into question the continued administration of mRNA vaccines, especially in low-risk populations.
103. The analysis by Yasmin et al. also presents evidence of vaccine-induced immune thrombocytopenia (VITT), a condition characterized by severe thrombotic events at unusual sites, such as the cerebral venous sinus and portal veins. The authors suggest that mRNA vaccines may induce autoimmune responses leading to platelet dysfunction, a hypothesis supported by post-mortem findings. The review notes that platelet factor 4 (PF4) antibodies—previously implicated in adenoviral vector vaccine-induced thrombosis—may also play a role in post-mRNA vaccine clotting disorders, underscoring the need for further investigation into these immune-mediated mechanisms. This systematic review presents strong evidence that mRNA vaccines pose significant cardiovascular risks, with a notable incidence of thrombosis, myocarditis, and stroke leading to hospitalizations and fatalities. The disproportionate burden of adverse events linked to BNT162b2, coupled with the mechanistic plausibility of vaccine-induced immune dysfunction, supports the petition’s call for immediate suspension of mRNA COVID-19 vaccines.
104. Adding to the weight of evidence, a systematic review by Knudsen and Prasad highlights a critical failure in the reporting of myocarditis risk following COVID-19 mRNA vaccination, demonstrating how inadequate stratification has led to an underestimation of the true risk faced by young males. The study reviewed 29 primary publications estimating post-vaccine myocarditis incidence and found that only 28% used all four key stratifiers—sex, age, dose number, and vaccine manufacturer. Meanwhile, nearly half of the studies (45%) used only one or zero stratifiers, leading to diluted risk estimates that obscured the high vulnerability of young males while inflating risk estimates for lower-risk groups. This systemic failure to properly stratify has major implications for vaccine policy, as it has likely led to the minimization of myocarditis concerns and the continuation of recommendations that expose the highest-risk demographic—young males under 40, particularly after a second mRNA vaccine dose—to unnecessary harm.[67]
105. The study’s findings reveal that when myocarditis incidence is stratified with all four variables, the rates are alarmingly high, ranging from 8.1 to 39 cases per 100,000 doses in young males. The highest reported incidences were found in males aged 12–17 after a second dose of the Pfizer vaccine, with rates as high as 39 per 100,000, while the Moderna vaccine posed the greatest risk to males aged 18–24, with rates of up to 30 per 100,000. In contrast, studies using fewer stratification factors reported much lower myocarditis rates—often below 5 per 100,000—misleading policymakers and the public into believing the condition was an exceptionally rare event. The study’s meta-regression confirmed a strong correlation between stratification granularity and reported myocarditis risk: studies that stratified data less precisely consistently reported lower incidence rates, reinforcing the conclusion that failure to properly segment the data has resulted in an underappreciation of the vaccine-induced myocarditis risk in young males.
106. This failure to properly stratify has had serious policy consequences. The study notes that 70% of the myocarditis studies examined did not adequately separate the highest-risk subgroup, meaning that public health officials may have overlooked the severity of this adverse effect when formulating vaccination strategies. While the CDC eventually acknowledged the risk of myocarditis in young males and recommended extending the dosing interval to reduce incidence, the study suggests that had proper stratification been used from the outset, more robust risk mitigation measures—such as targeted recommendations against second doses for young males—could have been implemented sooner. The study also points out that myocarditis rates in its analysis were substantially higher than those reported by VAERS, suggesting that passive surveillance systems may also be undercounting cases, further compounding the problem of risk minimization.
107. Moreover, the review highlights how myocarditis rates after mRNA vaccination are comparable to or exceed those seen after SARS-CoV-2 infection in young males, challenging the rationale for mass vaccination in this demographic. While myocarditis is a known complication of COVID-19, the study references data showing that in men under 40, the risk of myocarditis after a second dose of Moderna exceeds the excess myocarditis cases associated with SARS-CoV-2 infection. The CDC has frequently cited the risks of myocarditis from COVID-19 itself as justification for vaccination, but this study suggests that the vaccine-induced risk may be even greater, particularly for young males who are already at low risk for severe COVID-19 outcomes. The study also notes that estimates of post-infection myocarditis are inherently less precise than vaccine-related myocarditis due to issues in case ascertainment, whereas vaccine myocarditis risk is directly measurable from known doses administered, further strengthening the case that the post-vaccine risk has been systematically underestimated.
108. This systematic review provides compelling evidence that the failure to properly stratify myocarditis risk has directly contributed to flawed public health policies that continue to expose young males to a known and serious risk. The study supports the petition to suspend mRNA vaccines by demonstrating how inadequate data reporting and misleading aggregate risk estimates have obscured an important safety signal. Given that young males receiving second doses of mRNA vaccines face a myocarditis risk that appears to surpass that of COVID-19 itself, it is imperative that regulatory agencies reassess the cost-benefit equation for this demographic. Until risk is properly stratified and transparently communicated, continued administration of these mRNA vaccines to young males constitutes an unacceptable public health failure.
109. A systematic review and meta-analysis by Lai et al. (2022) provides critical evidence supporting the petition’s call for a reassessment of mRNA COVID-19 vaccine safety due to documented risks of peripheral nervous system (PNS) adverse events. This comprehensive analysis synthesized data from 15 large-scale cohort studies, encompassing more than 33 million individuals, to evaluate the incidence of neurological complications following mRNA vaccination. The study’s findings indicate a significant association between mRNA vaccines and increased risk of Bell’s palsy, while also identifying a concerning elevation in Guillain–Barré syndrome (GBS) risk with the BNT162b2 vaccine compared to mRNA-1273.[68]
110. The meta-analysis found a statistically significant increase in the incidence of Bell’s palsy following mRNA vaccination. The overall incidence rate was 31.08 cases per 100,000 persons (95% CI: 1.44–60.71), with a relative risk (Peto odds ratio, POR) of 1.36 (95% CI: 1.03–1.79) when compared to unvaccinated individuals. This marginal but statistically significant increase suggests that the immune response triggered by mRNA vaccines may contribute to transient dysfunction of the facial nerve, leading to Bell’s palsy. Notably, the study identified a higher risk of Bell’s palsy following BNT162b2 compared to mRNA-1273, with a pooled POR of 1.64 (95% CI: 1.41–1.90), demonstrating that Pfizer’s vaccine poses a more significant neurological risk.
111. Further stratification revealed that Bell’s palsy risk was highest after the first dose, with an incidence rate of 6.07 per 100,000 persons (95% CI: 3.49–8.65). This rate remained elevated, though slightly lower, after the second dose at 5.06 per 100,000 persons (95% CI: 1.97–8.16). The study’s findings confirm a distinct vaccine-associated risk that warrants further scrutiny, as Bell’s palsy can result in long-term morbidity, and its occurrence following vaccination raises concerns about immune-mediated neurological dysfunction.
112. Guillain–Barré syndrome, a severe autoimmune disorder leading to acute flaccid paralysis, was also analyzed in the study. A key finding was that the risk of GBS following BNT162b2 was significantly higher compared to mRNA-1273, with a pooled POR of 2.85 (95% CI: 1.61–5.04). This indicates that individuals receiving the Pfizer vaccine faced nearly three times the risk of developing GBS compared to those who received Moderna. The study also found an unusually large effect size when comparing GBS risk between BNT162b2 recipients and unvaccinated individuals, with a POR of 7.39 (95% CI: 0.15–372.38). Given that GBS is a potentially life-threatening condition requiring intensive medical care and long recovery periods, any increased risk associated with mRNA vaccination is a serious safety concern.
113. The study discusses plausible immunological mechanisms that could explain the observed neurological complications. It highlights that mRNA vaccines elicit a strong innate immune response, including the production of type 1 interferons, which have been implicated in autoimmune nerve damage. Elevated levels of interferons have been linked to both Bell’s palsy and GBS, suggesting that the vaccine-induced inflammatory response may trigger peripheral nerve injury in susceptible individuals. The study references cases where similar immune-mediated neuropathies have been observed following interferon therapy, further supporting this hypothesis.
114. Additionally, Lai et al. emphasize the possibility of underreporting and underestimation of these adverse events. Despite the large sample size analyzed, real-world data collection systems may not capture all vaccine-associated PNS disorders, particularly if mild or moderate cases go undiagnosed or unreported. The study’s authors call for long-term post-market surveillance and further research into the neurological safety profile of mRNA vaccines, particularly in high-risk populations.
115. The findings of this systematic review align with the petition’s argument that mRNA vaccines pose significant neurological risks that have not been adequately addressed by public health authorities. The demonstrated increase in Bell’s palsy cases and the elevated risk of GBS provide compelling evidence that the neurological safety of these vaccines requires urgent reevaluation. Given that these conditions can lead to prolonged disability and healthcare burdens, the failure to properly assess and communicate these risks represents a serious public health oversight.
116. The systematic review by Lai et al. provides robust, large-scale evidence that directly supports the petition’s call for a reassessment of mRNA vaccine safety. The documented increase in PNS adverse events highlights the need for an immediate and thorough review of vaccine-related neurological risks, ensuring that safety concerns are fully addressed. Overall, the meta-analysis by Lai et al. strengthens the petition’s argument that the safety profile of mRNA COVID-19 vaccines has not been adequately characterized, particularly in relation to peripheral nervous system disorders. The study serves as a compelling piece of evidence that justifies the petition’s demand for a suspension of mRNA vaccine recommendations until more comprehensive safety evaluations can be conducted.
117. The potent evidence from these systematic reviews and meta-analyses demonstrates a clear pattern of significantly elevated risks associated with mRNA COVID-19 vaccines, including myocarditis, thrombotic events, and peripheral nervous system disorders, which have been downplayed by the FDA and inadequately addressed. The failure to properly stratify risk has obscured the true incidence of myocarditis in young males, while mounting evidence of neurological complications underscores the urgent need for further investigation and transparent risk assessment. These findings reveal critical gaps in post-market surveillance and highlight the limitations of passive reporting systems that likely underestimate the true burden of vaccine-induced injuries. The weight of scientific data presented here leaves no room for complacency. The petition calls for an immediate suspension of mRNA COVID-19 vaccines until comprehensive, independent safety reviews are conducted. Anything less would constitute a failure of regulatory oversight and an abdication of responsibility to protect public health.
Observed Harms Outweigh Claimed Benefits
118. There are now at least six studies demonstrating that mRNA COVID-19 vaccines increase risk of infection:
Ioannou et al – Vaccine effectiveness against documented SARS-CoV-2 infection was -3.26% (95% CI, -6.78% to -0.22%), meaning vaccinated individuals had a statistically significant higher infection rate than the unvaccinated control group.[69]
Nakatani et al – Vaccinated individuals had an 85% increased odds of infection compared to the unvaccinated (OR = 1.85, 95% CI: 1.33–2.57).[70]
Eythorsson et al – Those who received two or more doses had a 42% higher risk of reinfection than those with one dose or less (95% CI: 1.13–1.78).[71]
Chemaitelly et al – The effectiveness of Pfizer-BioNTech (BNT162b2) against symptomatic BA.1 and BA.2 Omicron infections dropped from 46.6% and 51.7% (1–3 months post-dose) to -17.8% and -12.1% (≥7 months). Moderna (mRNA-1273) declined from 71.0% and 35.9% to -10.2% and -20.4% over the same period.[72]
Shrestha et al (Cleveland Clinic) – The risk of COVID-19 increased with the number of vaccine doses received. Individuals with one prior dose had a 107% higher risk (HR = 2.07, 95% CI: 1.70–2.52), while those with more than three doses faced a 253% higher risk (HR = 3.53, 95% CI: 2.97–4.20).[73]
Feldstein et al (CDC) – Children vaccinated with Pfizer-BioNTech without prior SARS-CoV-2 infection were 159% more likely to get infected (HR = 2.59, 95% CI: 1.27–5.28) and 257% more likely to develop symptomatic COVID-19 (HR = 3.57, 95% CI: 1.10–11.63) compared to unvaccinated children without prior infection.[74]
119. A landmark study by Mead et al. (2024) presents the following abstract, “The COVID-19 modified mRNA (modmRNA) lipid nanoparticle-based “vaccines” are not classical antigen-based vaccines but instead prodrugs informed by gene therapy technology. Of considerable note, these products have been linked to atypical adverse and serious adverse event profiles. As discussed in Part 1, health-related risks and drawbacks were drastically misreported and underreported in the Pfizer and Moderna trial evaluations of these genetic products. Now in Part 2, we examine the main structural and functional aspects of these injectables.”[75]
120. According to Part 1 of the study, “Re-analysis of the Pfizer trial data identified statistically significant increases in serious adverse events (SAEs) in the vaccine group. Numerous SAEs were identified following the Emergency Use Authorization (EUA), including death, cancer, cardiac events, and various autoimmune, hematological, reproductive, and neurological disorders. Furthermore, these products never underwent adequate safety and toxicological testing in accordance with previously established scientific standards. Among the other major topics addressed in this narrative review are the published analyses of serious harms to humans, quality control issues and process-related impurities, mechanisms underlying adverse events (AEs), the immunologic basis for vaccine inefficacy, and concerning mortality trends based on the registrational trial data. The risk-benefit imbalance substantiated by the evidence to date contraindicates further booster injections and suggests that, at a minimum, the mRNA injections should be removed from the childhood immunization program until proper safety and toxicological studies are conducted. Federal agency approval of the COVID-19 mRNA vaccines on a blanket-coverage population-wide basis had no support from an honest assessment of all relevant registrational data and commensurate consideration of risks versus benefits. Given the extensive, well-documented SAEs and unacceptably high harm-to-reward ratio, we urge governments to endorse a global moratorium on the modified mRNA products until all relevant questions pertaining to causality, residual DNA, and aberrant protein production are answered.”[76]
121. Critically, Part 2 of the study found, “The COVID-19 modmRNA injectable products introduce a unique set of biological challenges to the human body with the potential to induce an extensive range of adverse, crippling, and life-threatening effects. Based on the fact that there is no current method to quantify host (cell-based) spike protein production in vivo following injection with these prodrugs, there is no standard “dose”. This is in part due to differences in spike protein production output, which depends on cell metabolism and transfection efficiency. It is therefore difficult to predict adverse event profiles on an individual basis, but considering that millions of adults across the world have reported severe and serious adverse events in the context of these modmRNA COVID-19 products, valid concerns are raised regarding injection of infants and younger age groups for whom COVID-19 poses only minimal risks.”⁵⁰
122. This paper addresses “the process-related genetic impurities inherent in mass production of these products, and the potential risks posed by these contaminants,” categorizes “the principal adverse events associated with the modmRNA products with a brief systems-based synopsis of each of the six domains of potential harms: (1) cardiovascular, (2) neurological, (3) hematologic; (4) immunological, (5) oncological, and (6) reproductive, and concludes with a discussion of the primary public health and regulatory issues arising from this evidence-informed synthesis of the literature while reiterating “the urgency of imposing a global moratorium on the modmRNA-LNP-based platform.”⁵⁰
123. The following infographic from page 37 of this study visually depicts the negative risk-benefit analysis that results from honest assessment of the evidence and data. The imbalance between observed harms and claimed benefits necessitates the suspension and withdrawal of EUA and BLA licenses for these vaccines:
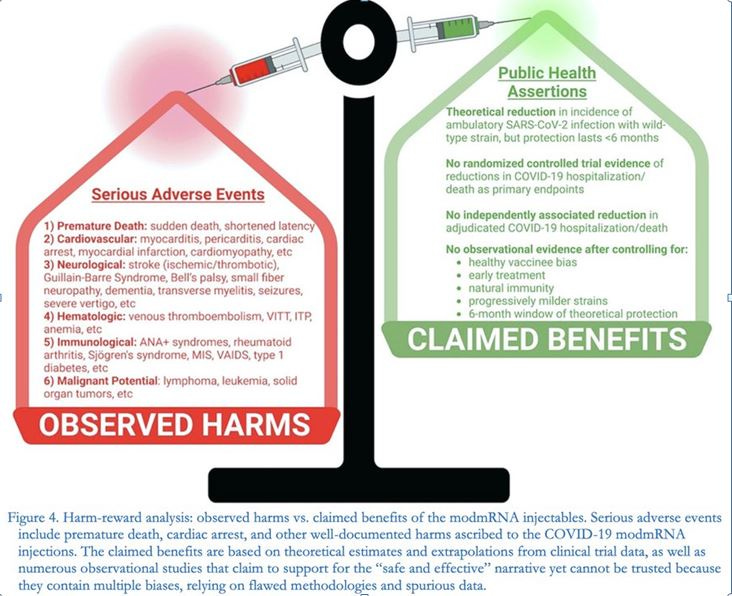
Counterarguments and Rebuttals
124. Our petition acknowledges that regulatory agencies, including the FDA, CDC, and WHO, have defended the continued use of mRNA COVID-19 vaccines based on their asserted safety and efficacy profiles. Below, we address the most common counterarguments and provide evidence-based rebuttals to strengthen the case for immediate suspension and ultimate withdrawal of EUA and BLA approvals.
125. Counterargument: "The Benefits of mRNA Vaccines Outweigh the Risks"
FDA Position:
The FDA maintains that while mRNA COVID-19 vaccines have associated risks (e.g., myocarditis, anaphylaxis), their benefits—including reduced hospitalization and mortality—outweigh the potential harms.
Public health officials argue that the risk of severe COVID-19, including long-term complications like "long COVID," is greater than the risks posed by vaccination.
Rebuttal:
Declining Benefit-Risk Ratio: While early clinical trials suggested a strong benefit-risk balance, real-world data now indicate declining vaccine efficacy and rising safety concerns. The risk of severe COVID-19 has substantially declined due to:
Widespread natural immunity.
The emergence of less severe SARS-CoV-2 variants.
Availability of alternative treatments (e.g., Paxlovid, monoclonal antibodies).
Disproportionate Risks for Young and Healthy Populations:
The benefit-risk calculus does not hold across all age groups.
For young males (16–29 years old), the risk of vaccine-induced myocarditis outweighs the risk of severe COVID-19.
Studies from Nordic countries, Israel, Ontario, and the U.S. military confirm significantly higher myocarditis rates than originally estimated (up to 1 in 3,772 for second-dose mRNA-1273).
No Reduction in Transmission:
Early claims that vaccines would prevent infection and transmission have been debunked.
The CDC and WHO have acknowledged that vaccinated individuals can still contract and spread COVID-19 at similar rates to the unvaccinated.
Thus, the assumption that all populations derive net benefits from mRNA vaccination is flawed.
126. Counterargument: "Severe Adverse Events Are Rare"
FDA Position:
The FDA asserts that severe vaccine-related adverse events are "extremely rare" and that the majority of reported events in VAERS are "coincidental" rather than caused by vaccination.
Regulatory agencies argue that myocarditis cases are "mild" and "self-resolving."
Rebuttal:
Underreporting Bias:
VAERS, EudraVigilance, and V-safe data suggest severe underreporting. The Lazarus Report (Harvard Pilgrim, 2010) estimated that VAERS captures fewer than 1% of actual vaccine adverse events.
Independent studies suggest that myocarditis cases could be significantly higher than what the FDA acknowledges.
Myocarditis Is Not "Mild" or "Self-Limiting":
Studies show myocardial scarring and long-term cardiac damage in affected individuals.
Autopsy data (Gill et al., 2023; Schwab et al., 2022) confirm fatal myocarditis cases post-mRNA vaccination.
A JAMA Cardiology study found over 20% of post-vaccine myocarditis cases result in persistent cardiac dysfunction.
Multiple Severe Adverse Events Beyond Myocarditis:
Neurological disorders: Bell’s Palsy, Guillain-Barré Syndrome, postural orthostatic tachycardia syndrome (POTS).
Autoimmune conditions: Lupus, rheumatoid arthritis, vaccine-induced immune thrombocytopenia.
Reproductive and fertility concerns: Biodistribution studies indicate mRNA accumulation in ovaries and testes, raising concerns about fertility impacts.
These findings challenge the narrative that vaccine adverse events are "rare" or "mild."
127. Counterargument: "VAERS Data Cannot Prove Causation"
FDA Position:
The FDA argues that VAERS is a passive surveillance system and cannot establish causation.
Rebuttal:
While VAERS is not designed to prove causation, it serves as an early warning system.
Many past vaccines (e.g., Rotavirus vaccine, Swine Flu vaccine, Dengvaxia) were withdrawn due to VAERS safety signals despite initial regulatory dismissals.
Pfizer’s own internal documents (released via FOIA) confirm that they identified over 1,200 deaths within the first three months of vaccine rollout—yet failed to act.
VAERS Trends Align with Independent Studies:
Multiple epidemiological studies corroborate VAERS data by confirming elevated myocarditis, pericarditis, and thrombotic events in vaccinated individuals.
The Global Vaccine Data Network (GVDN) study (2024) of 99 million vaccinated individuals found statistically significant increases in:
Neurological conditions: Bell’s Palsy, seizures, encephalitis.
Cardiovascular events: Myocarditis, pericarditis, pulmonary embolism.
Hematologic disorders: Thrombocytopenia, splanchnic vein thrombosis.
Historical Precedents for Regulatory Action Based on Passive Surveillance:
The 1976 Swine Flu vaccine was withdrawn after 53 deaths despite lack of definitive causality at the time.
The Rotavirus vaccine (RotaShield) was pulled due to a small number of intussusception cases.
COVID-19 vaccine-associated deaths far exceed these precedents for market withdrawal.
Thus, the sheer magnitude of VAERS-reported deaths demands urgent regulatory scrutiny, regardless of causality limitations.
128. Counterargument: "FDA Has Already Conducted Thorough Safety Reviews"
FDA Position:
The FDA asserts that post-marketing surveillance and existing safety studies are sufficient.
Rebuttal:
FDA Has Granted Unjustified Extensions on Post-Marketing Safety Studies:
Pfizer and Moderna failed to meet deadlines for critical myocarditis and reproductive safety studies.
The FDA granted multiple administrative extensions, delaying crucial safety evaluations.
If the vaccines are as safe as claimed, why are these studies delayed?
Emerging Data Shows Original Trials Were Incomplete or Flawed:
Pfizer’s pivotal trial unblinding compromised long-term efficacy and safety analysis.
The Biodistribution study revealed widespread mRNA circulation, contradicting early FDA claims.
FOIA documents show the FDA knew of serious adverse events early on but failed to act.
If the FDA’s prior safety reviews were truly sufficient, why do new safety signals keep emerging?
129. Counterargument: "Withdrawing mRNA Vaccines Is Irresponsible"
FDA Position:
The FDA will argue that withdrawing these vaccines could undermine confidence in public health institutions and leave vulnerable populations unprotected.
Rebuttal:
Protecting Public Health Requires Transparency and Accountability:
Regulatory agencies exist to protect people from harm, not to shield pharmaceutical companies from scrutiny.
FDA’s failure to enforce accountability undermines public trust far more than transparent reevaluation.
Safer Alternatives Exist:
Non-mRNA options (i.e. Novavax) provide alternative protection without the same risks.
Natural immunity is now widespread and robust in most populations.
Paxlovid and monoclonal antibody therapies are available for high-risk individuals.
Thus, withdrawal is not irresponsible—it is necessary to restore public trust in vaccine safety.
130. The premise that mRNA vaccines remain "safe and effective" across all populations is no longer supported by emerging data. The FDA’s past justifications for continued use have eroded in the face of real-world evidence. The precautionary principle and historical regulatory precedents demand that the FDA act decisively to suspend these vaccines and reassess their long-term safety.
Request for Withdrawal of Administrative Extensions
131. The seriousness and scope of adverse events attributed to mRNA warrants urgent and immediate administrative redress. In light of these well-documented harms, the administrative extensions granted to Moderna and Pfizer for critical postmarketing studies evaluating these harms must not be sustained.
A. Request for Immediate Action on Moderna’s Postmarketing Requirements
132. The petitioner respectfully requests that the FDA revoke the administrative extensions granted to Moderna for postmarketing requirements under the conditions outlined in its January 31, 2022, licensure approval letter. Specifically:
Deferred studies evaluating the safety and efficacy of SPIKEVAX in pediatric populations (Requirements 2, 4, and 8).
Safety studies assessing the incidence of myocarditis and other adverse events (Requirements 4, 5, 7, 9, and 12).
Observational studies of real-world effectiveness and pregnancy outcomes (Requirements 10 and 12).
Grounds for Revocation of Extensions
133. The failure to complete these studies within their original timelines delays essential safety and efficacy data, undermining the legal standards established under Section 351 of the Public Health Service Act.
· The administrative extensions compromise the timeliness and validity of critical safety data collection.
· Delayed studies fail to meet the FDA’s obligations to ensure public safety, particularly given the ongoing reports of severe adverse events linked to mRNA vaccines.
· The extensions disproportionately impact high-risk groups, such as pediatric and young adult populations, by delaying the evaluation of safety in these cohorts.
134. Relief Requested:
· Immediate revocation of administrative extensions for Requirements 2, 4, 5, 7, 8, 9, 10, and 12.
· Enforcement of the original deadlines stipulated in Moderna’s licensure approval.
B. Request for Immediate Action on Pfizer’s Postmarketing Requirements
135. The petitioner respectfully requests that the FDA revoke the administrative extensions granted to Pfizer for postmarketing requirements 5 and 6 under its August 23, 2021, licensure approval letter. Specifically:
· Requirement 5: Study C4591021, a post-conditional approval active surveillance study in Europe, evaluating the occurrence of myocarditis and pericarditis following administration of COMIRNATY.
· Requirement 6: Substudy of C4591021, describing the natural history of myocarditis and pericarditis following administration of COMIRNATY.
136. Grounds for Revocation of Extensions:
· Delay in Critical Safety Data:
— The extended timelines delay critical insights into myocarditis and pericarditis, particularly their long-term effects on vaccine recipients.
— These conditions have been widely reported as significant adverse events linked to mRNA COVID-19 vaccines, requiring immediate investigation.
· Compromised Public Health Protections:
— Delayed completion of safety studies leaves the public and healthcare providers without essential data to make informed decisions, particularly for vulnerable populations.
· Regulatory Integrity:
— Allowing continuous extensions undermines the FDA’s credibility and its statutory mandate to ensure the safety and efficacy of licensed biologics.
137. Relief Requested:
· Revoke the administrative extensions for postmarketing requirements 5 and 6.
· Enforce the original deadlines stipulated in Pfizer’s licensure approval.
138. The FDA’s failure to enforce timely completion of post-marketing safety studies violates its statutory duty under 21 U.S.C. § 355(k)(3). This federal statute mandates that the FDA must require and oversee the timely execution of post-marketing studies when safety concerns arise. By repeatedly granting unjustified extensions to Pfizer and Moderna for critical myocarditis, long-term safety, and effectiveness studies, the FDA has failed to uphold its legal obligations and has compromised public health.
139. Under 21 U.S.C. § 355(k)(3), the FDA does not have the discretion to indefinitely delay the completion of safety evaluations when they are essential to determining the risk profile of a product. Previous regulatory actions, such as the market withdrawals of Avandia and Vioxx due to delayed post-marketing safety data, demonstrate that such delays are grounds for immediate intervention. Yet, despite mounting evidence of severe adverse events—including myocarditis, pericarditis, neurological disorders, and immune system dysregulation—the FDA has permitted vaccine manufacturers to evade their legally required safety studies, leaving critical gaps in data needed for informed public health decisions.
140. The FDA’s failure to act has directly endangered millions of individuals who received these vaccines without access to the safety information that was legally required. Therefore, this petition demands that the FDA immediately revoke all administrative extensions granted to Pfizer and Moderna for incomplete post-marketing safety studies.
141. The final report of Florida’s Twenty-Second Statewide Grand Jury, which examined this very issue, came to the following conclusion: “These missed deadlines do not give us confidence. Each one represents an opportunity for the FDA and the public to be better informed about the safety of these products that cost billions of taxpayer dollars to develop, manufacture and administer. We recognize that conducting these trials and studies can be challenging work, but we think the money Pfizer and Medema made should be more than enough to fund and timely administer these tasks as they have been directed. The FDA would not speak to us directly, so we are not sure what their excuse would be for not holding Pfizer and Moderna's feet to the fire. Frankly, we are not sure any answer would satisfy us at this point, nor should it satisfy anyone else.”⁴³ The petitioner agrees with this assessment and urges the FDA to address these serious concerns by granting the relief requested.
Consideration of Alternatives and Why They Are Insufficient
142. In evaluating potential policy responses to the serious safety concerns associated with mRNA COVID-19 vaccines, it is important to consider less drastic alternatives than immediate suspension. While certain measures may provide partial solutions, they ultimately fail to adequately protect public health. The following options have been proposed as compromise solutions, yet each falls short in addressing the fundamental risks outlined in this petition.
Stronger Warnings for High-Risk Groups
143. One potential policy response is to issue stronger warnings for high-risk populations, particularly young males who face an elevated risk of vaccine-induced myocarditis and pericarditis. Regulatory agencies could amend product labeling to emphasize these risks, similar to how the FDA has included warnings for myocarditis in mRNA vaccine fact sheets.
144. While this measure would provide better informed consent, it is insufficient for several reasons. First, evidence suggests that young males are not the only group at elevated risk; neurological complications, thrombotic events, and autoimmune disorders have been reported across a broad demographic spectrum. Simply warning specific subpopulations does not address the systemic risks of mRNA vaccine technology. Second, labeling changes have limited practical impact in real-world settings. Many individuals do not read vaccine fact sheets in detail, and physicians often rely on public health guidance rather than fine-print warnings. Third, given the scale of reported adverse events, issuing stronger warnings while continuing to recommend widespread use of these vaccines could still result in significant harm.
A Moratorium on Boosters While Safety Data is Re-evaluated
145 Another proposed alternative is to impose a temporary moratorium on booster doses while further safety investigations are conducted. This approach would limit additional exposure while allowing regulators to reassess the long-term effects of repeated mRNA vaccination.
146. Although a moratorium on boosters would reduce ongoing risks, it does not address the continued administration of primary series vaccinations, particularly to individuals who may be at high risk of adverse events. Moreover, it fails to account for the fact that many adverse reactions have occurred even after initial doses, indicating that the concerns with these vaccines extend beyond repeated exposure. A booster pause would be a step in the right direction but would not resolve the underlying safety issues inherent to the platform itself.
Reforming Pharmacovigilance Reporting Standards
147. There is broad recognition that current pharmacovigilance systems, including VAERS and V-safe in the U.S. and EudraVigilance in the European Union, suffer from significant underreporting and data limitations. Strengthening adverse event reporting requirements, improving post-market surveillance, and conducting proactive safety investigations would enhance regulatory oversight and transparency.
148. However, while reforming pharmacovigilance is a necessary long-term goal, it does not provide an immediate safeguard against ongoing harms. The core issue is not merely that adverse events have been underreported but that existing data—despite its limitations—already demonstrates an alarming safety signal. The FDA, CDC, and WHO have not acted decisively despite overwhelming evidence from these systems. Relying on improved data collection mechanisms to justify continued administration of these vaccines assumes that more evidence is needed before taking precautionary action, when in reality, sufficient data already exists to warrant withdrawal.
149. Additionally, stronger pharmacovigilance mechanisms cannot retroactively prevent harm to those who have already suffered vaccine-related injuries. It is unethical to continue administering a product with known risks in the hope that better data collection will eventually clarify the full extent of those risks.
Providing Alternative Non-mRNA Vaccines as a Choice for Concerned Individuals
150. Offering non-mRNA COVID-19 vaccines, such as Novavax or traditional inactivated virus vaccines, as an alternative for those who do not wish to receive mRNA products is a commonly suggested solution. This approach would preserve vaccine availability while allowing individuals concerned about mRNA vaccine risks to opt for other formulations.
151. While expanding vaccine choice is generally positive, it does not resolve the core safety issues with mRNA vaccines. The continued recommendation of mRNA vaccines would mean that individuals, particularly those following official public health guidance, would still be exposed to their risks. Vulnerable groups, including children and those with preexisting conditions, may still be encouraged or required to receive mRNA vaccines due to existing mandates or workplace policies. Simply offering alternatives does not remove the systemic problems associated with the authorization and continued use of these products.
152. Furthermore, regulatory agencies have shown reluctance to promote non-mRNA vaccines on equal footing with mRNA options, raising questions about whether this approach would meaningfully reduce reliance on mRNA technology. Without an explicit suspension or withdrawal of mRNA vaccines, they would likely remain the dominant recommendation, leaving public health risks largely unmitigated.
153. Each of these proposed alternatives—stronger warnings, a booster moratorium, improved pharmacovigilance, and expanded vaccine choice—offers partial improvements but ultimately fails to address the fundamental issue: the continued availability of mRNA COVID-19 vaccines poses an unacceptable risk to public health. Given the scale and severity of reported adverse events, their widespread use cannot be justified by minor policy adjustments. Only immediate suspension and ultimate withdrawal of EUA and BLA approvals, coupled with a rigorous independent safety investigation, can restore confidence in the regulatory process and protect individuals from further harm.
Request for Reevaluation of Citizen Petition
(Docket Number FDA-2021-P-0460)
154. This petition has been drafted independently of earlier citizen petitions and reflects a contemporary response to the pressing issues surrounding COVID-19 vaccine safety and regulatory oversight. The petitioner only recently became aware of a 2021 citizen petition (FDA-2021-P-0460) after reading a January 17, 2025, New York Times article.[77] While this discovery was unanticipated, the petitioner was struck by the relevance of the concerns raised in the 2021 petition, which, in hindsight, appear prescient.
155. The 2021 petition raised foundational questions about the adequacy of the FDA’s safety monitoring, the integrity of its risk-benefit assessments, and its failure to address the legitimate uncertainties surrounding novel mRNA technology. It argued for a more cautious approach, emphasizing transparency, comprehensive data analysis, and the prioritization of informed consent. These issues remain as critical today as they were in 2021, yet they have taken on heightened urgency as real-world data has increasingly substantiated some of the petition’s warnings. For instance, the emergence of myocarditis, particularly among younger populations, and ongoing debates about the vaccines’ impact on natural immunity echo the concerns articulated in the earlier petition. Moreover, the evolving evidence base has underscored gaps in the FDA’s initial safety evaluations, revealing a troubling overconfidence in early trial data and post-market surveillance mechanisms.
156. In light of these developments, the 2021 petition serves not as a historical artifact but as a critical framework for understanding the regulatory missteps and oversight failures that continue to undermine public trust. Its emphasis on the inadequacies of passive surveillance systems, the lack of long-term safety data, and the dismissal of alternative approaches to managing COVID-19 remain central to the current effort. Where the 2021 petition sought to highlight emergent risks, the intervening years have transformed these risks into lived realities for many, demonstrating the tragic consequences of disregarding early warnings. This petition echoes the 2021 petition by incorporating the lessons of the past four years, situating its concerns within the broader context of evolving scientific knowledge, and advocating for a more accountable and transparent regulatory framework moving forward.
157. The relevance of the 2021 petition to today’s discourse cannot be overstated. Its prescience underscores the importance of addressing unresolved questions about vaccine safety, efficacy, and informed consent in a manner that reflects the accumulated evidence and lived experiences of those affected. By integrating the concerns raised in 2021 with contemporary findings, this petition seeks not only to hold regulatory bodies accountable but also to ensure that the mistakes of the past are not repeated as the public health community grapples with ongoing challenges and prepares for future crises.
Key Issues in the 2021 Petition
158. The 2021 petition raised a variety of concerns about COVID-19 vaccines authorized under Emergency Use Authorizations (EUAs) and requested several specific actions from the FDA. Below is a summary of the key issues:
A. Revocation of EUAs and Suspension of Approvals
The petition requested that the FDA revoke existing EUAs and refrain from granting further EUAs, NDAs, or BLAs for COVID-19 vaccines, arguing that the risks of serious adverse events and deaths outweighed the benefits.
It asserted that existing, approved drugs (e.g., ivermectin, hydroxychloroquine) were effective alternatives to COVID-19 vaccines, negating the need for EUAs.
B. Protection of Vulnerable Groups
Called for the FDA to:
Prohibit vaccine trials involving minors and revoke EUAs permitting vaccination of children under 16.
Revoke any tacit approval for use of COVID-19 vaccines in pregnant women and issue guidance against such use.
C. Alternative Treatments
Requested FDA action to amend guidance for using drugs such as hydroxychloroquine and ivermectin, claiming these were safe and effective against COVID-19 when used appropriately.
Criticized the FDA for its restrictive policies on these drugs, which it argued hindered early treatment options.
D. Vaccine Safety Concerns
Raised concerns about adverse events reported in the Vaccine Adverse Event Reporting System (VAERS), claiming unprecedented levels of deaths and injuries associated with COVID-19 vaccines.
Criticized the FDA and CDC for insufficient monitoring and public disclosure of safety data, despite having access to multiple safety databases.
Highlighted issues with animal studies and manufacturing processes, asserting that these inadequately assessed safety risks such as the distribution and persistence of lipid nanoparticles and spike protein production.
E. Effectiveness Concerns
Questioned the effectiveness of mRNA COVID-19 vaccines, citing breakthrough infections and data from the U.S. and U.K. suggesting efficacy issues.
Criticized the CDC for insufficient transparency and changes in how breakthrough cases were reported.
F. Misbranding
Alleged that describing COVID-19 vaccines as “safe and effective” violated FDA standards for investigational products, as such claims were inconsistent with EUA language.
G. Manufacturer Oversight and Quality Control
Expressed concerns about manufacturing quality issues, including problems with subcontractors such as Emergent BioSolutions, which had a history of regulatory violations.
H. Historical Precedents
Cited historical vaccine safety incidents (e.g., the 1976 swine flu vaccination campaign) as examples of the FDA acting to protect public health and called for similar action regarding COVID-19 vaccines.
15. The 2021 petition argued that the FDA had failed to uphold its mission to ensure the safety, efficacy, and accurate labeling of COVID-19 vaccines. It contended that the vaccines should not be promoted or approved until long-term safety and effectiveness were better established, and alternative treatments should be given greater emphasis.
How the New Petition Expands Upon the 2021 Petition
160. The 2021 petition and the new petition share several overlapping themes and arguments while the latter builds upon the earlier petition with expanded evidence.
A. Expanded Evidence Base:
· The new petition includes a significant accumulation of new data from peer-reviewed studies, pharmacovigilance systems, autopsy reports, and international findings, which were unavailable in 2021.
· It details emerging issues such as persistent spike protein, DNA contamination, and biodistribution of vaccine components, which add to systemic harm concerns.
B. Focus on Manufacturing and Batch Variability:
· The new petition cites manufacturing inconsistencies, such as batch-to-batch variability, contamination, and regulatory lapses, as critical concerns. It provides examples of stainless steel contaminants, DNA contamination, and deviations from Good Manufacturing Practices (GMP).
C. Post-Market Surveillance Failures:
· The new petition critiques post-marketing extensions granted to Pfizer and Moderna, arguing these delays have undermined the integrity of safety evaluations.
· It calls for revocation of these extensions to ensure timely and accurate safety assessments.
D. Legal and Administrative Developments:
· The new petition accounts for legal and regulatory changes since 2021, including the conclusion of the COVID-19 public health emergency and increased public scrutiny of vaccine safety.
· It references lawsuits, such as the Texas Attorney General’s case against Pfizer, and international advocacy efforts like The Hope Accord.
E. Public and Institutional Trust:
· The new petition addresses the erosion of public trust in regulatory bodies and calls for greater transparency to restore confidence in vaccine oversight.
F. Increased Scope of Harms:
· The new petition expands on systemic harms by detailing evidence of vascular, neurological, reproductive, and autoimmune conditions, along with long-term implications of mRNA and spike protein persistence.
G. International Context:
· The new petition incorporates global findings and advocacy efforts, highlighting support from international bodies like the World Council for Health and Doctors for COVID Ethics.
H. Call for Broader Accountability:
· The new petition explicitly critiques the FDA for regulatory lapses, calling for the suspension pending updated safety review and ultimate withdrawal of licensure for mRNA vaccines and stricter oversight of manufacturers.
161. Without intending to – because the new petition was drafted independently from the 2021 petition – the new petition builds on the foundational arguments of the 2021 petition, incorporating new scientific findings, regulatory failures, and broader advocacy efforts. While the core issues of safety, transparency, and risk-benefit evaluation remain central, the new petition reflects the evolving evidence base and public health landscape, making a more comprehensive and urgent case for immediate regulatory action.
Why Reevaluation of the 2021 Petition is Necessary
162. A reevaluation of the 2021 petition is critical in light of significant developments in scientific evidence, the regulatory environment, and the evolving public health landscape. These factors collectively underscore the urgency of revisiting the original concerns to ensure that vaccine safety, transparency, and regulatory integrity align with current knowledge and public health needs. Below, this argument is presented in depth.
Significant Accumulation of New Evidence
163. The body of scientific evidence since 2021 has grown substantially, strengthening the concerns raised in the original petition and providing new insights into the risks and inadequacies of mRNA COVID-19 vaccines. This includes:
a. Emerging Safety Concerns:
Persistent Spike Protein and mRNA:
n Studies have revealed that vaccine-derived spike proteins and mRNA persist in tissues for weeks to months, contradicting earlier assurances that they degrade rapidly. Persistent spike protein has been associated with inflammation, tissue damage, and immune dysregulation.
n Examples: Research by Röltgen et al. (2022) and Patterson et al. (2022) documenting the presence of spike proteins in the brain, heart, and other vital organs for extended periods.
Expanded Adverse Event Data:
n Pharmacovigilance systems like VAERS, EudraVigilance, and VigiBase have reported a sharp increase in severe adverse events, including myocarditis, pericarditis, and neurological conditions. The volume and severity of reported cases far exceed historical safety thresholds for other vaccines.
n Specific findings, such as myocarditis rates among young males (up to 1 in 3,772 for some subgroups), necessitate a reevaluation of risk-benefit analyses.
b. Manufacturing and Batch Variability:
Investigations have identified batch-to-batch variability in mRNA vaccines, leading to inconsistencies in efficacy and safety. Contaminants such as stainless steel and DNA fragments in certain batches, as reported by regulatory agencies and independent researchers, further compromise safety assurances.
c. Real-World Effectiveness and Waning Immunity:
Evidence of waning immunity and the inability of mRNA vaccines to prevent transmission of newer SARS-CoV-2 variants undermines their initial justifications under EUA and BLA standards.
Studies showing the rapid decline in vaccine efficacy and the emergence of vaccine-resistant variants emphasize the need for a more nuanced evaluation of benefits versus risks.
d. New Research Corroborating Systemic Harms:
Peer-reviewed studies and international reports have documented links between mRNA vaccines and systemic harms such as autoimmunity, chronic inflammation, and potential DNA integration due to residual plasmid DNA contamination. These findings were not available in 2021 but substantiate many concerns raised in the original petition.
164. Changes in the Regulatory Environment
a. End of the Public Health Emergency:
The declared COVID-19 public health emergency, which justified the original Emergency Use Authorizations (EUAs), has ended. SARS-CoV-2 has transitioned to endemicity, with hospitalization and mortality rates significantly reduced. This shift invalidates the emergency conditions under which mRNA vaccines were initially authorized.
b. Availability of Alternatives:
Since 2021, non-mRNA COVID-19 vaccines, FDA-approved antiviral therapies (e.g., Paxlovid), and monoclonal antibodies have become widely available, fulfilling the "adequate, approved, and available alternatives" criterion under the EUA framework. The continued deployment of mRNA vaccines under EUA is no longer justified in this context.
c. Failure to Meet Post-Marketing Requirements:
Pfizer and Moderna have failed to meet critical post-marketing study deadlines, including evaluations of myocarditis and other safety concerns. The FDA’s decision to grant administrative extensions undermines the urgency and accountability required for such evaluations.
These delays further erode public trust in regulatory oversight and leave unresolved safety questions unaddressed.
d. Legal and Institutional Scrutiny:
The regulatory landscape has been shaped by lawsuits (e.g., the Texas Attorney General's case against Pfizer) and public demands for transparency, including calls for the disclosure of safety signal investigations. Reevaluating the 2021 petition would demonstrate the FDA's commitment to accountability and public trust.
165. Shifts in the Public Health Landscape
a. Decline in COVID-19 Severity:
COVID-19 has shifted from a pandemic to an endemic disease, with milder clinical outcomes in most populations. Vaccination strategies that were justifiable in the pandemic’s early phases are no longer appropriate given the reduced threat level.
b. Erosion of Public Trust:
Public skepticism toward mRNA vaccines has grown due to inconsistent messaging, lack of transparency, and high-profile safety concerns. A reevaluation of the 2021 petition provides an opportunity to restore confidence by addressing these concerns comprehensively and transparently.
c. Long-Term Safety Implications:
As mRNA vaccines were developed and deployed under emergency circumstances, their long-term safety profile remains uncertain. Emerging evidence of potential chronic health issues, such as autoimmune disorders and cardiovascular complications, heightens the need for retrospective safety assessments.
d. Focus on Subpopulations:
The risks of mRNA vaccines for specific subpopulations—such as young males (myocarditis risk), children, and pregnant women—have become clearer since 2021. Reevaluating the original petition allows for targeted regulatory action to protect these vulnerable groups.
166. Ethical and Regulatory Imperatives
a. Precautionary Principle:
The precautionary principle, a cornerstone of public health ethics, mandates that products with potential for significant harm should be withdrawn or restricted until their safety is conclusively established. The mounting evidence of adverse events and systemic harms necessitates such an approach.
b. Transparency and Accountability:
Reevaluating the 2021 petition would signal a commitment to transparency and rigorous oversight, addressing public concerns about conflicts of interest and regulatory capture.
c. Alignment with Current Evidence:
Regulatory decisions should evolve with the evidence base. The concerns raised in 2021 have been corroborated and expanded upon by subsequent findings, making it essential to revisit the original arguments with updated data.
167. The necessity of reevaluating the 2021 petition is underscored by the substantial new evidence, changes in the regulatory environment, and shifts in the public health landscape. The issues raised in the original petition have not only been validated but also amplified by subsequent developments, making a fresh review both scientifically and ethically imperative. Reevaluating the 2021 petition would:
Address unresolved safety concerns with the benefit of a significantly expanded evidence base.
Align regulatory decisions with the current public health context, including the availability of safer alternatives and the conclusion of the public health emergency.
Demonstrate the FDA’s commitment to accountability, transparency, and public trust.
By undertaking a rigorous and transparent reevaluation, the FDA can fulfill its statutory mandate to protect public health, rebuild confidence in regulatory oversight, and ensure that vaccine policies are informed by the latest and most comprehensive scientific evidence.
168. Furthermore, the FDA's 2021 response to the citizen petition contained several significant flaws that undermine its arguments and conclusions. These flaws are more visible in 2025 than they may have been at the time. First, the agency relied heavily on general assertions of safety and efficacy without adequately addressing critical gaps in data, particularly regarding long-term risks associated with the novel mRNA technology. These shortcomings were especially troubling given the rapid deployment of COVID-19 vaccines under Emergency Use Authorizations (EUAs), which inherently involve less comprehensive pre-authorization testing. The FDA's dismissal of concerns about specific adverse events, such as myocarditis and thrombosis with thrombocytopenia, rested on incomplete or premature data analysis, often sidestepping robust risk-benefit evaluations for sensitive populations such as children, adolescents, and pregnant women.
169. The FDA’s approach to pediatric vaccination was particularly problematic. It justified EUAs for children and adolescents based on general public health benefits rather than clear evidence of individual benefit outweighing risks in this population. Children, who have a much lower risk of severe COVID-19, were subjected to potential vaccine-related adverse events, including myocarditis, without the FDA adequately addressing why these risks were acceptable in light of their extremely limited susceptibility to severe disease. Furthermore, the agency’s reliance on clinical trial data, which excluded key subpopulations and lacked long-term follow-up, highlighted an overconfidence in preliminary findings while ignoring calls for more targeted studies.
170. Another critical weakness in the FDA response was its dismissal of alternative therapeutics and preventive measures. The agency argued that no adequate, approved alternatives to the vaccines existed but failed to consider evolving scientific literature on therapeutics such as ivermectin and hydroxychloroquine. By framing its analysis in a way that dismissed any potential merit in these alternatives, the FDA left the impression of bias rather than an open evaluation of all available options. This stance also ignored broader public health approaches, such as improving population-level immunity through natural exposure or integrating vaccine use with non-pharmaceutical interventions.
171. The FDA’s arguments also suffered from a lack of transparency and accountability. For example, while it claimed that the known and potential benefits of vaccination outweighed the risks, it did not provide sufficient public access to the raw data underlying these conclusions. This opacity prevented independent verification and undermined public trust in the agency’s findings. Additionally, the FDA failed to explain why it did not convene independent advisory committees to reassess vaccine safety and efficacy as new data became available, particularly as concerns about adverse events mounted.
172. Finally, the FDA's approach to contraindications and pregnancy guidance revealed an inconsistent application of regulatory standards. Despite acknowledging the lack of comprehensive data on the safety of vaccines in pregnant women, the FDA did not include contraindications or sufficiently detailed warnings in its labeling. Instead, it dismissed the petitioner’s concerns by asserting that the risks did not "clearly outweigh any possible therapeutic benefit," a conclusion that lacked rigorous evidentiary support. This pattern of downplaying uncertainty while overstating certainty in its conclusions about safety and efficacy was a recurring theme in the FDA’s response.
173. The request to reevaluate the 2021 petition underscores the continuity of concerns about mRNA COVID-19 vaccine safety, efficacy, and regulatory oversight. The prescience of the earlier petition, now validated by subsequent evidence, reveals how critical gaps in safety monitoring and risk assessment have persisted. These unresolved issues demand immediate regulatory intervention. By revisiting the 2021 petition in light of new findings, this petition aims to address systemic regulatory failures and ensure that the lessons of the past are applied to prevent further harm. The recommendations presented herein, including the suspension and withdrawal of EUA and BLA approvals and the implementation of enhanced safety evaluations, represent an urgent and necessary response to these ongoing concerns. This holistic approach not only safeguards public health but also rebuilds trust in the FDA’s commitment to transparency and accountability.
Acknowledgment of the Complementarity of Citizen Petition (Docket Number 2025-P-0335-0001)
174. This petition is submitted with the central objective of ensuring transparency, accountability, and decisive regulatory action regarding the documented harms caused by mRNA COVID-19 vaccines. While the primary focus remains on the overwhelming safety concerns and the need for immediate policy responses to protect public health, it is essential to recognize the critical work undertaken by other petitioners who have highlighted additional regulatory failures and legal violations surrounding these products.
175. On January 31, 2025, this petitioner became aware of another petition entitled “Petition for Administrative Action Regarding COVID-19 modRNA Vaccines of Pfizer & Moderna,” filed on January 21, 2025, with Docket Number 2025-P-0335-0001, which presents a powerful and meticulously argued case for the immediate revocation or suspension of the biologics license applications (BLAs) and emergency use authorizations (EUAs) for Pfizer-BioNTech’s Comirnaty and Moderna’s Spikevax. The petition raises urgent concerns including:
A. Wrongful and Illegal Categorical Exclusions from Environmental Assessments (EAs) – The petition documents how Pfizer and Moderna were improperly granted categorical exclusions from required environmental assessments under 21 CFR 25.31, thereby evading the legally mandated review of these products by the Cellular, Tissue, and Gene Therapies Advisory Committee (CTGTAC). This misclassification prevented critical scrutiny of the mRNA-LNP technology under the appropriate regulatory framework for gene therapies.
B. Excessive Synthetic DNA Contamination – The petition presents substantial evidence from multiple independent laboratories, including one supervised by FDA scientists, confirming that Pfizer and Moderna’s products contain synthetic DNA contamination at levels vastly exceeding regulatory safety thresholds. Furthermore, it highlights concerns about the presence of SV40 promoter and enhancer sequences, which have implications for genomic integration and oncogenic risk.
C. Regulatory and Legal Failures in Product Classification and Informed Consent – The petition demonstrates that, despite meeting the FDA’s own criteria for gene therapy products, mRNA COVID-19 vaccines were wrongfully classified as traditional vaccines rather than gene therapies, thus bypassing critical oversight mechanisms. This misclassification not only enabled procedural shortcuts in the approval process but also contributed to the failure to ensure full public disclosure and legally valid informed consent.
176. While the current petition does not duplicate the legal and regulatory arguments outlined in 2025-P-0335-0001, we fully acknowledge their validity and importance. The core focus of our petition remains on the urgent need to reassess and halt the continued use of mRNA COVID-19 vaccines based on the widespread and severe harms they have caused. However, the regulatory violations identified in 2025-P-0335-0001 provide crucial context for understanding how these products were rushed into widespread use without proper oversight.
177. Given the complementary nature of these efforts, we strongly urge the FDA and the Department of Health and Human Services to consider both petitions together. The arguments presented in 2025-P-0335-0001 reinforce the necessity of the actions demanded in this petition: a comprehensive safety reassessment, full transparency of COVID-19 vaccine-related harms, and immediate corrective measures to prevent further injury to the public. Together, these petitions present an irrefutable case for urgent regulatory intervention.
Regulatory Capture and Need for Independent Oversight
178. A growing body of evidence demonstrates that corporate actors routinely manipulate the scientific and regulatory process to protect their commercial interests at the expense of public health. This practice—sometimes referred to as the "disinformation playbook"—has been extensively documented in industries such as tobacco, pharmaceuticals, and chemicals. The tactics used to suppress unfavorable scientific findings, delay regulatory action, and manufacture public uncertainty about health risks bear striking similarities across industries, including the current response to safety concerns surrounding mRNA COVID-19 vaccines.
179. As detailed in “The Disinformation Playbook: How Industry Manipulates the Science-Policy Process—and How to Restore Scientific Integrity,” Reed et al. (2021) describe five primary tactics that corporations use to control the scientific and regulatory discourse:
A. Faking Science – Funding biased studies or suppressing unfavorable research
Manufacturing Uncertainty – Questioning the credibility of independent science
Harassing Scientists – Targeting and silencing dissenting experts
Buying Credibility – Using respected institutions to push corporate narratives
Manipulating Government Officials – Infiltrating and influencing regulatory agencies
Each of these tactics is relevant to the concerns raised in this petition, as evidence suggests that Pfizer and Moderna have engaged in similar behaviors to suppress scrutiny of their mRNA COVID-19 vaccines.
180. Reed et al. describe how corporations often fund studies with methodologies designed to produce favorable results or suppress negative findings. “Industry-sponsored research is more likely to have favorable outcomes for the target product or process than research funded by other sources, a phenomenon known as the ‘funding effect’.”[78]
181. The petition highlights that both Pfizer and Moderna have failed to disclose critical safety data. Their clinical trials excluded key populations, including individuals with autoimmune conditions and prior vaccine-related adverse reactions, and postmarket surveillance data has been selectively reported. This aligns with the tactics Reed et al. describe, where companies “hide conflicts of interest for industry-funded or -affiliated scientists who publish papers, give testimony, or comment publicly” and “interfere with studies during the prepublication process, including peer review.”
182. Furthermore, safety signals identified in real-world data, such as increased rates of myocarditis and pericarditis, have been downplayed or dismissed outright by vaccine manufacturers. This is consistent with historical corporate strategies where companies “publish studies with flawed methodologies or bury studies with unfavorable results.” The need for an independent review of the full dataset—including unpublished or suppressed safety signals—is paramount.
183. Another common industry tactic is the deliberate sowing of uncertainty around legitimate scientific findings. “Companies can overemphasize scientific uncertainty through public relations campaigns, features in media outlets, political lobbying, or comments in regulatory dockets,” Reed et al. explain. “Often, companies target a single offending study for undermining their objectives.”
184. The petition documents how similar tactics have been employed by Pfizer and Moderna in response to studies demonstrating increased risks of myocarditis, neurological disorders, and other adverse events associated with their mRNA vaccines. Studies showing a higher-than-reported incidence of myocarditis, such as the Hong Kong Epidemiology of Acute Myocarditis/Pericarditis Study, have been ignored or dismissed as “outliers.” Similarly, the Florida Department of Health’s independent analysis, which recommended against mRNA vaccines for young males, was met with public attacks rather than scientific engagement. These responses are emblematic of the disinformation playbook's strategy to “turn principles of transparency against science.”
185. The playbook also includes efforts to intimidate and discredit scientists who present evidence contrary to corporate narratives. As Reed et al. note, corporations routinely “accuse scientists of scientific misconduct or attack their credibility” and “harass scientists by abusing open-records requests or subpoenas.”
186. Multiple scientists who have raised concerns about vaccine safety—including cardiologists, immunologists, and pharmacovigilance experts—have reported facing professional censure, reputational attacks, and funding withdrawals. The intense backlash against whistleblowers within Pfizer itself, as well as independent researchers who questioned trial data integrity, mirrors historical cases of corporate suppression of inconvenient scientific findings.
187. One of the most alarming patterns outlined in the disinformation playbook is the way corporations embed themselves within regulatory agencies, ensuring favorable treatment. Reed et al. detail how “industries routinely wield their financial power to influence elected officials to co-craft industry-friendly policies, exploit gaps or weaknesses in regulatory schema, or stymie unfavorable regulations.”
188. The revolving door between the FDA, CDC, and pharmaceutical companies is well-documented. Many decision-makers overseeing mRNA vaccine approvals and regulatory decisions have direct financial ties to the very companies they are supposed to regulate. This has created a climate in which postmarket safety concerns are downplayed, independent reviews are obstructed, and regulatory scrutiny is insufficient. The FDA’s failure to enforce timely completion of Pfizer and Moderna’s postmarketing safety studies, allowing repeated deadline extensions, could be perceived as an indicator of regulatory capture.
Request for Independent Safety Review
189. The evidence outlined in The Disinformation Playbook provides an essential context for understanding why mRNA COVID-19 vaccines must be subject to immediate suspension and independent review. The documented strategies used by pharmaceutical companies to suppress inconvenient safety data, manufacture uncertainty, and exert undue influence over regulatory agencies raise serious concerns about the reliability of industry-reported vaccine safety profiles.
190. Given this historical precedent and the mounting safety concerns documented in this petition, the FDA must take immediate corrective action. The petition calls for:
A. The suspension of mRNA COVID-19 vaccine licensure pending an independent safety review.
An immediate investigation into the suppression of safety signals by vaccine manufacturers.
The implementation of stronger safeguards against regulatory capture and conflicts of interest in vaccine oversight.
191. The petitioner requests the establishment of an independent, third-party safety review board, appointed by the Commissioner, composed of:
Independent experts in vaccinology, epidemiology, cardiology, neurology, immunology, and toxicology with no financial or professional conflicts of interest with vaccine manufacturers.
Regulatory and legal experts to assess whether Pfizer-BioNTech and Moderna have complied with all postmarketing safety requirements.
Public representation, including at least one individual with lived experience of vaccine injury or a qualified advocate for vaccine safety, to ensure transparency, accountability, and inclusion of affected communities in regulatory decision-making.
192. The Independent Safety Review Board should be tasked with the following:
A. Conducting a comprehensive, independent review of safety data, including long-term follow-up studies, biodistribution data, and autopsy findings.
Assessing pharmacovigilance signals and determining whether adverse events have been adequately investigated and addressed.
Investigating manufacturing inconsistencies and batch variability, which may explain disparities in reported adverse events.
Reviewing clinical trial data, including previously undisclosed or reclassified adverse events, to determine whether safety risks were minimized in regulatory filings.
Issuing advisory recommendations on whether EUA and BLA approvals should be revoked based on evidence of safety risks.
193. The board’s findings should be fully disclosed to the public in full transparency. Without these measures, the FDA risks repeating the mistakes of past regulatory failures, in which corporate interests were prioritized over public safety. The integrity of the scientific and regulatory process depends on rigorous, transparent, and independent oversight—free from industry manipulation.
Request for Mandatory Disclosure and Public Release of Safety Data
194. Under 21 U.S.C. § 355(l)(1), the FDA is required to make postmarket safety data publicly available. However, key safety signals have remained undisclosed or inadequately investigated. Full transparency is essential to restore public trust. In order to restore public trust and ensure regulatory transparency, the petitioner requests:
195. Mandatory Disclosure of All Validated Safety Signals
Require Pfizer and Moderna to publicly disclose all validated safety signals, including those that were dismissed, and the methodologies used to investigate them.
Publish comprehensive details of the safety signal validation process, including:
Timelines,
Criteria for validation,
Justifications for conclusions.
196. Public Release of Safety Signal Methodologies and Findings
Direct Pfizer and Moderna to provide detailed reports on all safety signals investigated as part of their Global Safety Databases (GSDs), including signals identified through:
VAERS
V-safe
EudraVigilance
VigiBase
Make these reports publicly available to ensure transparency in regulatory decisions.
197. Retrospective Review of Refuted Safety Signals
Conduct an independent review of all safety signals that were dismissed by Pfizer-BioNTech and Moderna to assess whether:
Sufficient evidence and methodological rigor were applied.
Any valid safety concerns were inappropriately disregarded.
· Publish the findings of this review and require corrective action if necessary.
Request for Internal HHS Investigation into Potential Fraudulent Misrepresentation and Willful Misconduct by mRNA COVID-19 Vaccine Manufacturers (Prior to DOJ Referral)
198. In light of the DOJ Civil Division’s historical deference to regulatory agencies in matters concerning pharmaceutical fraud, this petition further requests that the Department of Health and Human Services (HHS) initiate an internal investigation into potential fraudulent misrepresentation and willful misconduct by Pfizer and Moderna prior to referring the matter to the Department of Justice (DOJ). Given the DOJ’s reluctance to pursue cases without prior regulatory agency findings, an internal fraud investigation by HHS will ensure that a referral is procedurally strong and backed by credible evidence gathered through an official agency review.
Legal Basis for HHS Investigation
199. HHS has a statutory duty under 21 U.S.C. § 355(e) and 42 U.S.C. § 247d-6d to ensure that biologics and other medical countermeasures remain compliant with federal safety and efficacy standards. Furthermore, under the Inspector General Act of 1978 (5 U.S.C. App. 3), the HHS Office of Inspector General (OIG) has the authority and the statutory duty to investigate allegations of fraud involving federally funded programs, including those related to COVID-19 vaccine development and procurement. OIG investigation is not discretionary but mandatory under this statutory framework.
200. Given that Pfizer and Moderna received significant federal funding under Operation Warp Speed and government procurement contracts, HHS has an obligation to investigate whether these manufacturers knowingly engaged in fraudulent misrepresentation in their interactions with the FDA, the Centers for Disease Control and Prevention (CDC), and other federal agencies.
Legal Basis for Referral
201. While the PREP Act grants liability immunity for covered countermeasures during a declared public health emergency, it explicitly excludes cases of willful misconduct. The statute defines willful misconduct as an act that:
A. Was undertaken to achieve a wrongful purpose;
Was committed knowingly without legal or factual justification; and
Disregarded a known or obvious risk that was so great it was highly probable harm would occur (42 U.S.C. § 247d-6d(c)(3)).
202. Additionally, the False Claims Act (31 U.S.C. § 3729) prohibits companies from defrauding the federal government by making false statements to obtain funding. Evidence suggests that Pfizer and Moderna engaged in fraudulent misrepresentation to secure Emergency Use Authorization (EUA) and subsequent Biologics License Application (BLA) approvals, including:
Misrepresentation of Clinical Trial Safety Data – Exclusion of critical adverse event reports and improper trial data handling.
Failure to Disclose Known Adverse Events – Concealment of myocarditis risks, potential DNA contamination, and immune dysregulation.
False Marketing as “Safe and Effective” – Continued public messaging that misrepresented known risks despite emerging safety concerns.
203. The DOJ has exclusive enforcement power over the False Claims Act and the willful misconduct exemption under the PREP Act. HHS and the FDA lack the authority to directly enforce these laws but are obligated to refer credible evidence of violations to the DOJ.
Petition Request: HHS Fraud Investigation Prior to DOJ Referral
204. This petition formally requests that:
A. HHS initiate an internal fraud investigation and review all available evidence to determine whether Pfizer and Moderna engaged in willful misconduct and fraudulent misrepresentation in securing EUA and BLA approvals for their COVID-19 mRNA vaccines.
The HHS Office of Inspector General (OIG) conduct an independent audit of clinical trial data submissions, adverse event reporting, and internal communications between vaccine manufacturers and federal agencies to assess whether critical safety data was knowingly withheld or manipulated.
HHS compile a formal investigatory report with findings to provide an official regulatory basis for DOJ action.
Upon completion of the investigation, HHS refer the case to the DOJ for enforcement under the False Claims Act (31 U.S.C. §§ 3729-3733) and the willful misconduct exemption under the PREP Act (42 U.S.C. § 247d-6d) if cause to proceed is found.
Evidence Suggesting Potential Fraud and/or Willful Misconduct
205. In November 2021, for example, The BMJ published an article based on revelations from Brook Jackson, a former regional director at Ventavia Research Group, a subcontractor involved in Pfizer's pivotal phase III COVID-19 vaccine trial.[79] Jackson reported that the company falsified data, unblinded patients, employed inadequately trained vaccinators, and was slow to follow up on adverse events. Despite notifying her superiors and filing a complaint with the U.S. Food and Drug Administration (FDA), she was terminated the same day. These allegations suggest intentional actions to obscure critical safety data during the vaccine trial process.
206. Jackson’s whistleblower lawsuit, filed under the False Claims Act (FCA), was dismissed by the U.S. District Court for the Eastern District of Texas on procedural grounds—primarily due to the government’s continued purchase of Pfizer’s vaccine, which the court interpreted as undermining the materiality requirement of the FCA.[80] However, this dismissal does not preclude a renewed federal investigation by the Department of Health and Human Services (HHS), which could uncover additional evidence warranting DOJ intervention.
207. The dismissal was based on legal technicalities rather than a determination of factual accuracy. The materiality standard under the FCA was interpreted narrowly, given that the government continued purchasing Pfizer’s vaccine despite Jackson’s allegations. No evidentiary trial or discovery process was conducted to validate or refute her claims. The case was dismissed without prejudice as to the U.S. government, meaning federal agencies (HHS, DOJ) retain the right to investigate and take legal action if new evidence emerges. A new administration, with a focus on transparency and accountability, can revisit the FDA’s handling of Jackson’s allegations.
208. Brook Jackson’s allegations remain a credible and serious concern that were not fully examined in her dismissed False Claims Act lawsuit. An HHS-led investigation into Pfizer’s clinical trial practices, if properly executed, could uncover sufficient evidence for DOJ intervention, congressional hearings, and major regulatory reforms. Given the gravity of potential fraudulent conduct in the approval process of a vaccine mandated for millions, this petitioner strongly recommends initiating a formal internal investigation within HHS. This will not only hold Pfizer accountable if wrongdoing is found but also ensure that future vaccine trials meet the highest standards of safety and transparency.
209. Statutory Authority Under the FCA: Specifically, the False Claims Act (31 U.S.C. §3729) imposes liability on any person who:
· "Knowingly presents, or causes to be presented, a false or fraudulent claim for payment or approval" (31 U.S.C. §3729(a)(1)(A)).
· "Knowingly makes, uses, or causes to be made or used, a false record or statement material to a false or fraudulent claim" (31 U.S.C. §3729(a)(1)(B)).
· "Conspires to commit a violation" of the FCA (31 U.S.C. §3729(a)(1)(C)).
210. Materiality Argument: The Supreme Court’s ruling in Universal Health Services, Inc. v. United States ex rel. Escobar, 579 U.S. 176 (2016), established that misrepresentations are material if they have a natural tendency to influence, or are capable of influencing, government payment decisions—even if the government continues making payments after becoming aware of the fraud.[81] Here, fraudulent trial data could have significantly impacted regulatory approval and vaccine purchases by the government, strengthening the case for FCA applicability.
211. “Materiality, like knowledge, cabins the Act’s falsity requirement. As the Supreme Court has explained, not every false statement is actionable; only those likely to induce an unwitting government payment or forbearance. The parties asked the Supreme Court in Escobar whether for False Claims Act purposes a statement, true on its face, could be made false by omission. The Court held that “liability can attach when the defendant submits a claim for payment that makes specific representation about the goods or services provided but knowingly fails to disclose the defendant’s violation of a material statutory, regulatory, or contractual requirement.” Escobar has supplied later courts with factors to assist in the determination of whether a false statement is material…” explained the Congressional Research Service in the seminal 2021 report, “Qui Tam: The False Claims Act and Related Federal Statutes.”[82]
212. Given this precedent, if it can be demonstrated that fraudulent clinical trial data influenced the FDA’s regulatory decisions regarding Emergency Use Authorization (EUA) or full approval of COVID-19 vaccines, there is a strong argument that False Claims Act liability could apply. If drug manufacturers knowingly submitted falsified or misleading clinical trial data to the FDA (e.g., suppressing adverse event data or overstating efficacy) this could be deemed material under Escobar. FDA approval and EUA decisions were crucial in enabling pharmaceutical companies to receive billions of dollars in government contracts and vaccine purchases.
213. The U.S. government directly funded the research, development, and procurement of COVID-19 vaccines through Operation Warp Speed and other mechanisms. If the vaccines would not have been purchased, distributed, or mandated had the government been aware of falsified data, the materiality threshold is satisfied. Escobar held that continued government payments do not automatically negate materiality if the government was unaware of fraud at the time of initial decisions. If evidence exists that regulators had limited or no knowledge of data manipulation during approval but later discovered it, this strengthens the FCA case.
214. Given the gravity of these allegations, it is imperative that the Department of Health and Human Services (HHS) conducts a thorough internal investigation to assess the extent of potential misconduct and fraudulent misrepresentation by vaccine manufacturers, as well as determining what the government knew during the approval process and when the government knew it.
215. While no known cases exist of the PREP Act’s willful misconduct exemption being successfully invoked to revoke liability immunity for a vaccine manufacturer, precedent for DOJ enforcement against pharmaceutical companies engaged in fraudulent misrepresentation, data falsification, and deceptive marketing is well established. This petition urges federal agencies to treat vaccine manufacturers engaging in similar conduct with the same level of scrutiny and enforcement as past corporate fraud cases involving government-funded medical products.
216. The following historical cases provide strong parallels for DOJ intervention and prosecution when a pharmaceutical company engages in fraudulent misrepresentation while benefiting from federal contracts and funding:
· GlaxoSmithKline’s $3 Billion Fraud Settlement (2012)
In 2012, GlaxoSmithKline (GSK) reached a $3 billion settlement with the Department of Justice (DOJ) for fraud, misrepresenting safety data, and off-label marketing of multiple prescription drugs. As part of this settlement, GSK:
· Knowingly concealed safety data related to the antidepressant Paxil, which was marketed for use in children despite internal evidence of increased suicide risk.
· Misrepresented clinical trial data for Avandia, a diabetes drug, by failing to disclose heart attack risks.
· Engaged in deceptive marketing practices that resulted in false claims to federal healthcare programs, leading to liability under the False Claims Act (FCA) (31 U.S.C. §§ 3729-3733).
This case demonstrates that deliberate suppression of safety risks and fraudulent misrepresentation of drug safety data constitute prosecutable offenses, even when the product in question was previously approved by the FDA. Pfizer and Moderna’s failure to disclose myocarditis risks, DNA contamination, and adverse immune responses in their clinical trial data mirrors GSK’s misconduct and warrants similar legal scrutiny.
· Pfizer’s $2.3 Billion DOJ Settlement for Off-Label Marketing Fraud (2009)
In 2009, Pfizer entered into a $2.3 billion settlement with the DOJ, marking the largest healthcare fraud settlement in U.S. history at the time. The charges against Pfizer included:
· Illegal promotion and off-label marketing of Bextra, an anti-inflammatory drug, for uses not approved by the FDA.
· Providing false safety information to healthcare providers and government agencies.
· Knowingly misrepresenting drug efficacy and safety while securing federal contracts.
This case establishes that Pfizer has a documented history of engaging in fraudulent conduct involving government contracts and regulatory agencies. Given the emerging evidence that Pfizer knowingly misrepresented safety data related to its COVID-19 vaccine, including myocarditis risks and potential long-term adverse effects, the DOJ must be compelled to investigate whether the company has repeated similar fraudulent practices.
217. This petition argues that Pfizer and Moderna’s conduct aligns with the fraudulent actions pursued by the DOJ in the GlaxoSmithKline and Pfizer settlements in the following ways:
Knowingly Concealing Safety Risks: Evidence suggests that both Pfizer and Moderna failed to disclose critical safety concerns, including myocarditis risks, potential DNA contamination, and immune system dysregulation.
Misrepresenting Clinical Trial Data: Whistleblower testimony, FOIA-released documents, and internal communications indicate potential data manipulation, including underreporting of adverse events.
Deceptive Marketing of “Safe and Effective” Messaging: Despite internal awareness of emerging safety concerns, both manufacturers continued promoting their vaccines as unconditionally “safe and effective,” influencing public health policy and mandates.
218. Given these parallels, HHS and the FDA must conduct a fraud investigation into Pfizer and Moderna before referring the case to the DOJ to ensure procedural strength in enforcing False Claims Act violations and the willful misconduct exemption under the PREP Act.
219. Regulatory agencies exist to ensure that medical products meet the highest standards of safety, efficacy, and transparency. The findings outlined in this petition raise serious concerns that these standards were not met in the case of COVID-19 mRNA vaccines. Historically, failures to address regulatory missteps—whether in the cases of Vioxx, thalidomide, or the Tuskegee syphilis experiments—have led to significant harm, loss of public trust, and subsequent reforms.
220. The evidence presented necessitates a thorough review. An internal HHS investigation would provide the regulatory foundation necessary for DOJ enforcement actions, ensuring compliance with statutory protections against fraudulent misrepresentation. If HHS and FDA fail to act on this matter, it will not only call into question their commitment to regulatory integrity but may also prompt further external scrutiny from Congressional oversight bodies, independent investigations, and legal challenges.
221. Given the scale of federal funding involved, the public health implications, and the need for confidence in regulatory institutions, it is imperative that HHS initiate an internal fraud investigation into the clinical trial practices, data integrity, and regulatory disclosures of Pfizer and Moderna. This petition does not call for premature conclusions, but rather for an objective and transparent process to assess whether regulatory misrepresentation occurred and, if so, what corrective actions are warranted under existing legal frameworks.
Conclusion
222. The evidence presented in this petition underscores significant and mounting concerns regarding the safety, efficacy, and oversight of mRNA COVID-19 vaccines. While these vaccines were developed and deployed under extraordinary circumstances, the emerging data on systemic harms, manufacturing inconsistencies, and post-market surveillance failures demand urgent regulatory reassessment.
223. The following key findings form the basis of this petition:
A. Unprecedented Safety Signals: Peer-reviewed studies, pharmacovigilance data, and real-world evidence have identified severe adverse events, including myocarditis, pericarditis, and neurological disorders, at rates that far exceed historical safety thresholds for other vaccines. The systemic harms linked to prolonged spike protein persistence and biodistribution further amplify these risks.
B. Inadequate Oversight: The failure to complete critical post-marketing safety studies within original timelines undermines the integrity of regulatory processes. Administrative extensions granted to Pfizer and Moderna delay essential safety evaluations, leaving the public vulnerable to unknown risks.
C. Erosion of Trust: Lack of transparency regarding validated safety signals and incomplete disclosure of safety signal investigations have significantly eroded public confidence in both the vaccines and the regulatory institutions tasked with ensuring their safety.
D. Availability of Safer Alternatives: The original EUA criteria—predicated on the absence of adequate, approved, or available alternatives—are no longer satisfied. FDA-approved non-mRNA vaccines and effective therapeutics now provide safer options for COVID-19 prevention and treatment.
224. This petition respectfully but emphatically calls upon the FDA, HHS, and CBER to exercise their statutory authority and duty to protect public health by:
Withdrawing the Emergency Use Authorizations and Biologics Licenses for Pfizer-BioNTech and Moderna’s mRNA COVID-19 vaccines.
Enforcing compliance with post-marketing safety study timelines and revoking administrative extensions that compromise timely safety evaluations.
Mandating transparency and public reporting on safety signal investigations and findings.
225. The withdrawal of these vaccines is not merely a precautionary measure but an ethical and regulatory imperative. It reflects a commitment to prioritizing public safety, rebuilding trust in the regulatory process, and setting a higher standard for future vaccine development and oversight.
226. This petition joins a growing chorus of voices, including the following doctors' groups and organizations calling for the withdrawal of mRNA COVID-19 vaccines:
A. World Council for Health (WCH)
Call for Withdrawal: WCH issued a statement calling for the immediate stop to COVID-19 vaccinations, declaring them dangerous and unsafe for human use.
Pharmacovigilance Report: Published a report highlighting a concerning safety signal with the vaccines based on pharmacovigilance databases. (https://www.worldcouncilforhealth.org/covid-19-vaccine-pharmacovigilance-report/) (see Appendix B)
B. Association of American Physicians and Surgeons (AAPS)
Call for Withdrawal: AAPS has called for the complete market withdrawal of all COVID-19 vaccines and boosters, deeming them unsafe for human use. (see Appendix E)
C. Doctors for COVID Ethics (D4CE)
Call for Moratorium: D4CE has called for a global moratorium on the use of these vaccines, citing ethical and safety concerns. (see Appendix F)
D. The Hope Accord
Petition for Suspension: The Hope Accord has a petition calling for the "immediate suspension" of mRNA COVID vaccines, supported by various high-profile doctors. (see Appendix D)
E. Florida’s Surgeon General
Statement: Florida's Surgeon General has publicly called for a halt to the use of mRNA vaccines due to safety concerns. (see Appendix G)
F. National Citizens Inquiry (NCI)
Evidence-Based Consensus: After interviewing experts, NCI has called for the market removal of all COVID-19 vaccines, concluding they are unsafe for human use. https://nationalcitizensinquiry.ca/national-citizens-inquiry-recommends-immediate-halt-to-covid-19-vaccinations/
227. On November 25, 2024, a “notice of extreme concern about COVID-19 modified mRNA vaccine safety and quality” was issued by an international consortium of medical and other professionals from numerous European countries, Canada, and the United States demanding an immediate suspension of COVID-19 mRNA vaccines, citing serious health concerns. With over 600 international signatories, the letter states:
· Scientific evidence shows that it was a lottery as to which batch a person received and the side effects – including death – they experienced.
· COVID-19 vaccines were never tested for their ability to block transmission. Thus, medical product regulators, as well as government agencies, misinformed and even misled the public when coercing them into accepting these products
· Multiple independent analyses have shown that modified mRNA vaccines contain variable but alarmingly high levels of residual DNA. This raises extreme concerns about the risks to human health and the potential for genetic damage that were not accounted for scientifically in the authorization process.
228. Finally, on January 28, 2025, even as this petitioner had nearly completed the drafting of this petition, a new peer-reviewed manuscript was published in Science, Public Health Policy and the Law, calling for COVID-19 vaccines to be removed from human use. The paper, a comprehensive review of publicly issued calls for market removal of COVID-19 vaccines by physicians, scientists, researchers, and others, reiterates many of the points made in this petition. The paper’s abstract states:
COVID-19 vaccination campaigns around the globe have failed to meet fundamental standards of safety and efficacy, leading to mounting evidence of significant harm. More than 81,000 physicians, scientists, researchers, and concerned citizens, 240 elected government officials, 17 professional public health and physician organizations, 2 State Republican Parties, 17 Republican Party County Committees, and 6 scientific studies from across the world have called for the market withdrawal of COVID-19 vaccines. As of September 6, 2024, the CDC has documented 19,028 deaths in the United States reported to the Vaccine Adverse Event Reporting System (VAERS) by healthcare professionals or pharmaceutical companies who believe the product is related to the death. The total number of COVID-19 vaccine deaths reported to VAERS (37,544 among all participating countries) have far exceeded the recall limits of past vaccine withdrawals by up to 375,340%. The criteria for an FDA Class I recall, which applies to products with a reasonable probability of causing serious adverse health consequences or death, have been far exceeded. Excess mortality, negative efficacy, widespread DNA contamination, and a lack of demonstrated reduction in transmission, hospitalization, or mortality have undermined the rationale for continued administration. These unified requests for regulatory action underscore substantial shortcomings in data safety monitoring and risk mitigation. Immediate removal of COVID-19 vaccines from the market is essential to prevent further loss of life and ensure next steps are taken for accountability of the harm incurred.[83]
229. The paper includes the following table detailing the voluminous calls for COVID-19 vaccine market withdrawal, only some of which we have previously discussed in this petition:
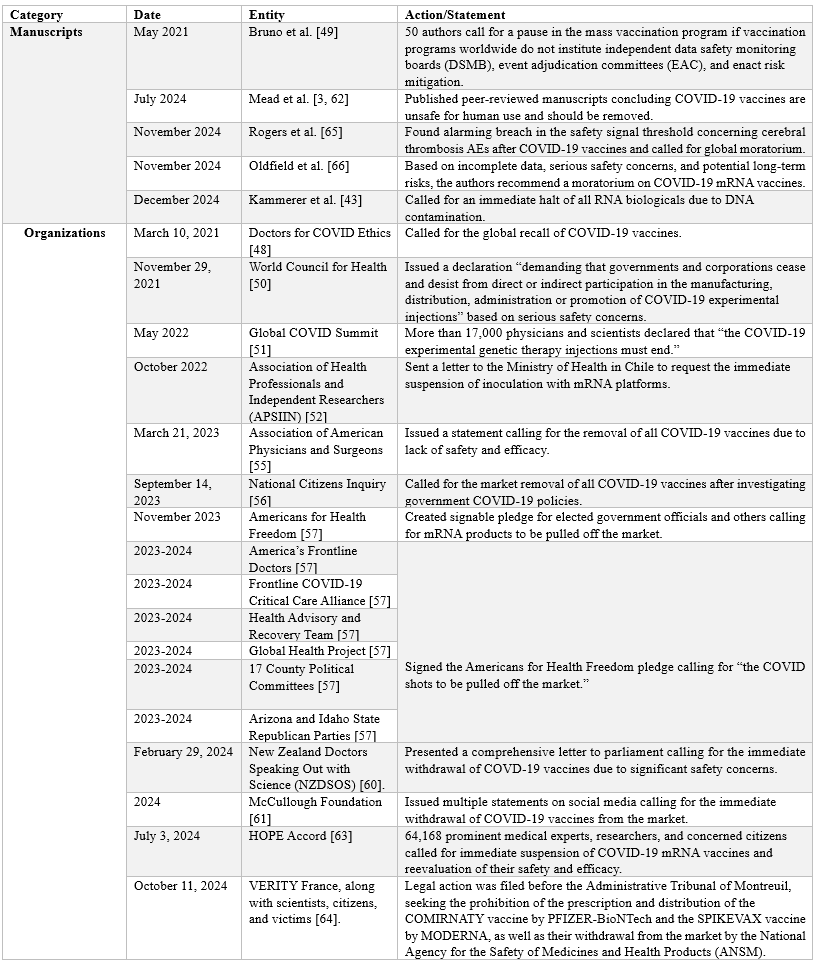

230. The paper concludes, “We expect that calls for an immediate moratorium on COVID-19 vaccines will continue to increase until a critical mass is reached, and the products are finally removed from the market. Excess mortality, negative efficacy, and widespread DNA contamination associated with COVID-19 vaccines have been sufficiently demonstrated. The FDA’s criteria for a Class I recall have been far exceeded. No large-scale, conclusive, randomized, double-blind, placebo-controlled trials have demonstrated reduction in infection transmission, hospitalization, or death as primary endpoints. Thus, the COVID-19 vaccines are not proven to be effective in reducing important clinical outcomes. A position supporting COVID-19 vaccination goes against good medical practice and violates the Hippocratic Oath to above all, do no harm. Immediate removal of COVID-19 vaccines from the market is essential to prevent further loss of life and ensure the next steps for accountability are taken.”⁵⁰
231. This petition represents the voices of countless individuals—vaccine recipients, healthcare professionals, researchers, and concerned citizens—united in their demand for accountability and transparency. Public health depends on the confidence that medical interventions are both safe and effective, and this confidence cannot be sustained without rigorous regulatory oversight.
232. Here is a final review of the sequence of actions requested:
Step 1: Immediate Suspension of EUAs and BLAs for mRNA COVID-19 Vaccines
(Prevent further harm while a review is conducted.)
Step 2: Establishment of an Independent Safety Review Board
(Ensure safety analysis is independent, unbiased and rigorous.)
Step 3: Revocation of Administrative Extensions for Postmarketing Requirements
(Compel completion of critical safety studies before making a final determination.)
Step 4: Revocation of EUA and BLA Approvals if Safety Review Confirms Risks
(Decide on full revocation based on completed pharmacovigilance data.)
Step 5: Mandatory Disclosure and Public Release of Safety Data
(Ensure transparency for public trust.)
Step 6: Re-evaluation of FDA-2021-P-0460 Petition
(Assess prior regulatory missteps to prevent recurrence.)
Step 7: Internal HHS Investigation and Referral to DOJ
(Holding actors accountable for fraud and misconduct.)
233. The petitioner requests that the Secretary of Health and Human Services exercise direct oversight over this petition due to the critical nature of the safety concerns raised. Given prior regulatory failures and unresolved conflicts of interest within FDA leadership, it is in the public interest that this matter be reviewed at the highest administrative levels within HHS.
234. In light of these ethical concerns, the petitioner requests that all determinations regarding this petition be made by the Secretary of Health and Human Services, the incoming FDA Commissioner upon confirmation by the U.S. Senate, or other designated officials within HHS who are free from conflicts of interest.
235. The petitioner urges the Secretary of Health and Human Services and other designated officials to act decisively and without undue delay in addressing the serious harms outlined in this petition by granting the relief requested.
C. ENVIRONMENTAL IMPACT
The undersigned hereby states that the relief requested in this petition will have no
environmental impact and therefore an environmental assessment is not required under 21 C.F.R.
Sections 25.30 and 25.31.
D. ECONOMIC IMPACT
Economic impact information will be submitted upon request of the Commissioner.
E. CERTIFICATION
The undersigned certifies that, to the best of their knowledge and belief, this petition includes all information and views upon which the petition relies, and that it includes representative data and information known to the petitioner that are unfavorable to the petition.
The Petitioner therefore respectfully urges that this request be granted forthwith.
Respectfully submitted,
/s/ Ethan Augreen
Citizens MAHA
Appendix A – Annotated References
Portions of this petition rely on the work of independent researchers who compiled the mRNA Vaccine Biodistribution, Persistence, and Adjuvant Toxicity Library.
Compiled by Dr. Martin Wucher, MSC Dent Sc (eq DDS), Dr. Byram Bridle, PhD, Erik Sass, et al. (last updated December 26, 2024.) Doi: https://zenodo.org/records/14559625
Description of the library
Originally part of the outer coat of the SARS-CoV2 virus, where it functions as a “key” to “unlock” (infect) cells, spike proteins are also produced in large amounts by the mRNA “vaccines,” triggering a short-lived immune response in the form of antibodies. However, a growing body of evidence has shown that the spike protein is harmful by itself (see: “Spike protein pathogenicity research library,” https://zenodo.org/records/14559644). Furthermore, research has demonstrated that:
1) Both the “vaccine” mRNA encoding for the spike protein antigen and the spike protein itself can penetrate distant tissues, causing systemic harms.
2) “Vaccine” mRNA and the spike protein antigen persist in the tissues of human vaccine recipients and animal test subjects far longer than claimed by public health officials, while viral spike proteins have been shown to persist even longer.
3) The ionizable lipid nanoparticles (LNPs) used in the experimental mRNA injections are highly inflammatory on their own, including their polyethylene glycol (PEG) component, an established cause of anaphylaxis (an extreme allergic reaction).
The following research collection presents over 100 peer-reviewed studies documenting I) the wide distribution and II) persistence of “vaccine” mRNA and the encoded spike protein, as well as III) the potential harms of the LNP delivery system (some studies with overlapping findings appear in more than one category). Taken together with evidence of the spike protein’s pathogenicity (https://zenodo.org/records/14559644), these findings suggest that the mRNA “vaccines” can distribute harmful, long-lasting spike protein uncontrollably throughout the body, causing injuries and death by various means.
Please note that a small number of studies in section I) investigate the ability of viral spike protein resulting from infection to cross important physiological barriers on its own, while some studies in section II) demonstrate the long persistence of viral-derived spike protein in the absence of viable virus, bolstering concerns about the identical “vaccine” spike.
I. Spike protein and “vaccine” mRNA biodistribution
Compiled by Dr. Martin Wucher, MSC Dent Sc (eq DDS), Erik Sass, et al.
Biodistribution studies show that both the “vaccine” mRNA encoding for the spike protein antigen and the spike protein itself can penetrate distant tissues, causing systemic harms to a variety of organs and organ systems, including the placenta. The following research collection presents over 50 peer-reviewed studies (n=54) documenting the wide distribution of “vaccine” mRNA and the associated spike protein throughout human beings and animal test subjects.
These articles confirm that “vaccine” mRNA and spike protein can reach tissues and organs including the heart, liver, brain, lungs, placenta, umbilical cord, breast milk, lymph nodes, thymus, kidneys, spleen, bladder, large intestine, eyes, adrenal glands, ovaries, testes, bone marrow, skin, lacrimal glands, and appendix. Additionally, a small number of studies demonstrate the viral spike protein’s ability to cross important physiological barriers independently of the rest of the virus, suggesting identical “vaccine”-derived spike protein can do the same.
1. Australian Government Department of Health—Therapeutic Goods Administration, “Nonclinical evaluation of BNT162b2 [mRNA] COVID-19 vaccine (COMIRNATY),” 2021, Available from: https://www.tga.gov.au/sites/default/files/foi-2389-06.pdf
• “Lipid nanoparticle formulation… and encapsulation efficiency similar to LNP in BNT162b2 vaccine… distribution mainly into liver, adrenal glands, spleen and ovaries over 48 h.”
2. Bansal S et al., “Cutting Edge: Circulating Exosomes with COVID Spike Protein Are Induced by BNT162b2 (Pfizer-BioNTech) Vaccination prior to Development of Antibodies: A Novel Mechanism for Immune Activation by mRNA Vaccines,” J. Immunol. 2021, 207, 10: 2405–2410. doi: https://doi.org/10.4049/jimmunol.2100637
• plasma
3. Baumeier C et al., “Intramyocardial Inflammation after COVID-19 Vaccination: An Endomyocardial Biopsy-Proven Case Series,” Int. J. Mol. Sci. 2022, 23, 13: 6940.
doi: https://doi.org/10.3390/ijms23136940
• “The expression of SARS-CoV-2 spike protein within the heart and the dominance of CD4+ lymphocytic infiltrates indicate an autoimmunological response to the vaccination.”
4. Boros LG et al., “Long-lasting, biochemically modified mRNA, and its frameshifted recombinant spike proteins in human tissues and circulation after COVID-19 vaccination,” Pharmacol Res Perspect 2024, 12, 3: e1218. doi: https://doi.org/10.1002/prp2.1218
• “… clinical studies now report that modified SARS-CoV-2 mRNA routinely persist up to a month from injection and can be detected in cardiac and skeletal muscle at sites of inflammation and fibrosis, while the recombinant spike protein may persist a little over half a year in blood.”
5. Brady M et al., “Spike protein multiorgan tropism suppressed by antibodies targeting SARS-CoV-2,” Comm. Biol. 2021, 4, 1318. doi: https://doi.org/10.1038/s42003-021-02856-x
• After intravenous injection, “SP had a body-wide biodistribution, slow regional elimination, except for the liver, which showed an accumulation, and differential organ uptake. SP uptake was highest for the lungs and this was followed by the kidney, heart, and liver, but lowest in the brain.”
6. Brogna C et al., “Detection of recombinant Spike protein in the blood of individuals vaccinated against SARS-CoV-2: Possible molecular mechanisms,” Proteonomics Clin App. 2023, 17, 6. doi: https://doi.org/10.1002/prca.202300048
• plasma
7. Broudic K et al., “Nonclinical safety assessment of an mRNA Covid-19 vaccine candidate following repeated administrations and biodistribution,” J. Appl. Toxicol. 2024, 44, 3: 371-390. doi: https://doi.org/10.1002/jat.4548
• lymph nodes, spleen, liver, lacrimal glands, brain, thymus, lungs, adrenal glands, bone marrow, kidneys, testes, ovaries
8. Burkhardt A, “Pathology Conference: Vaccine-Induced Spike Protein Production in the Brain, Organs etc., now Proven.” Report24.news, 2022, available online: https://report24.news/pathologie-konferenz-impfinduzierte-spike-produktion-in-gehirn-u-a-organen-nun-erwiesen/
• Heart, brain, liver, appendix, bronchi, skin, spleen
9. Buzhdygan TP et al., “The SARS-CoV-2 spike protein alters barrier function in 2D static and 3D microfluidic in-vitro models of the human blood–brain barrier,” Neurobiol Dis. 2020m 146: 105131. doi: https://doi.org/10.1016/j.nbd.2020.105131
10. Castruita JAS et al., “SARS-CoV-2 spike mRNA vaccine sequences circulate in blood up to 28 days after COVID-19 vaccination,” APMIS 2023, 131: 128–132. doi: https://doi.org/10.1111/apm.13294
• plasma
11. Cosentino M and Franca Marino, “Understanding the Pharmacology of COVID- 19 mRNA Vaccines: Playing Dice with the Spike?” Int. J. Mol. Sci. 2022, 23, 18: 10881. doi: https://doi.org/10.3390/ijms231810881
• “Taken as a whole, evidence strongly supports the possible link between inappropriate expression of S protein in sensitive tissues and subsequent tissue damage.”
12. DeOre BJ et al., “SARS-CoV-2 Spike Protein Disrupts Blood-Brain Barrier Integrity via RhoA Activation,” J Neuroimmune Pharmacol. 2021, 16, 4:722-728. Doi: https://doi.org/10.1007/s11481-021-10029-0
13. Di J et al., “Biodistribution and Non-linear Gene Expression of mRNA LNPs Affected by Delivery Route and Particle Size,” Pharm Res 2022, 39: 105-114. doi: https://doi.org/10.1007/s11095-022-03166-5
• liver, spleen, muscle, and inguinal lymph nodes
14. European Medicines Agency, Assessment Report, available online: https://www.ema.europa.eu/en/documents/assessment-report/comirnaty-epar-public-assessment-report_en.pdf
• “Synthetic mRNAs encapsulated in LNPs can reach many organs, such as the spleen, heart, kidneys, lungs and brain. The mRNAs were found in the ovaries and the testicles in small quantities, during the biodistribution studies of this vaccine after 9 days.”
15. European Medicines Agency, COVID-19 Vaccine Moderna, available online: https://www.ema.europa.eu/en/documents/assessment-report/spikevax-previously-covid-19-vaccine-moderna-epar-public-assessment-report_en.pdf
• Vaccine mRNAs are detectable in a wide variety of organs: brain, heart, lungs, eyes, gonads.
16. Fertig TE et al., “Beyond the injection site: identifying the cellular targets of mRNA vaccines,” J Cell Ident 2024, 3, 1. doi: https://www.cellidentity.org/wp-content/uploads/2024/06/JoCI_003-Reviews_003_Fertig_MRNa.pdf
• Overview of studies showing wide distribution throughout the body.
17. Fertig TE et al., “Vaccine mRNA Can Be Detected in Blood at 15 Days Post Vaccination,” Biomedicines 2022, 10, 7: 1538. doi: https://doi.org/10.3390/biomedicines10071538
• plasma
18. Hanna N et al. “Biodistribution of mRNA COVID-19 vaccines in human breast milk,” eBioMedicine 2023, 96, 104800. doi: 10.1016/j.ebiom.2023.104800 https://pubmed.ncbi.nlm.nih.gov/37734205/
• “Of 13 lactating women receiving the vaccine (20 exposures), trace mRNA amounts were detected in 10 exposures up to 45 h post-vaccination. “
19. Hano S et al., “A case of persistent, confluent maculopapular erythema following a COVID-19 mRNA vaccination is possibly associated with the intralesional spike protein expressed by vascular endothelial cells and eccrine glands in the deep dermis,” J Dermatol 2023, 50, 9: 1208-1212. doi: https://doi.org/10.1111/1346-8138.16816
• “Surprisingly, immunohistochemical staining of the lesion 100 days after the disease onset revealed the COVID-19 spike protein expressed by vascular endothelial cells and eccrine glands in the deep dermis. As she had no episode of COVID-19 infection, it is highly likely that the spike protein was derived from the mRNA vaccine and it might be the cause of the development and persistence of her skin lesions.”
20. Hulscher N et al., “Autopsy findings in cases of fatal COVID-19 vaccine-induced myocarditis,” ESC Heart Failure 2024. doi: https://doi.org/10.1002/ehf2.14680
• “COVID-19 vaccine Spike protein is produced in the body for an uncontrolled duration and in unknown quantity resulting in deleterious effects, especially on the heart, explaining the cardiovascular deaths seen in our study without evidence of other organ system involvement.”
21. Judicial Watch, “JW v HHS FDA Pfizer BioNTech Vaccine prod 3 02418,” March 21, 2022, https://www.judicialwatch.org/documents/jw-v-hhs-fda-pfizer-biontech-vaccine-prod-3-02418/
• LNP biodistribution to liver, spleen, adrenal glands, ovaries. “Outside the injection site, low levels of radioactivity were detected in most tissues, with the greatest levels in plasma observed 1-4 hours post-dose.”
22. Kammala AK et al., “In vitro mRNA-S maternal vaccination induced altered immune regulation at the maternal-fetal interface,” Am. J. Reprod. Immunol. 2024, 91, 5: e13861. doi: https://doi.org/10.1111/aji.13861
• “… our study indicates that mRNA-S-based maternal vaccination during pregnancy may influence the maternal-fetal interface's COVID-19 interaction and immune regulation. Further investigation is warranted to assess safety and implications.”
23. Kawano H et al., “Fulminant Myocarditis 24 Days after Coronavirus Disease Messenger Ribonucleic Acid Vaccination,” Intern. Med. 2022, 61, 15: 2319-2325. doi: https://doi.org/10.2169/internalmedicine.9800-22
• “… positive immunostaining for severe acute respiratory syndrome coronavirus 2 spike protein and C4d in the myocardium."
24. Kent SJ et al., “Blood Distribution of SARS-CoV-2 Lipid Nanoparticle mRNA Vaccine in Humans,” ACS Nano 2024, 18, 39: 27077-27089. doi: https://doi.org/10.1021/acsnano.4c11652
• “The similar kinetics of intact mRNA and the ionizable lipid in blood and the slow degradation of the mRNA suggest that mRNA lipid nanoparticles remain intact and travel from injection sites or lymph nodes into the bloodstream within 4 h postvaccination. The rapid dissemination of mRNA lipid nanoparticles in blood found in our study is consistent with the recent findings on the detection of mRNA in breast milk at 3−45 h postvaccination.”
25. Krauson AM et al., “Duration of SARS-CoV-2 mRNA vaccine persistence and factors associated with cardiac involvement in recently vaccinated patients,” npj Vaccines, 8, 141. doi: https://doi.org/10.1038/s41541-023-00742-7
• axillary lymph nodes, myocardium
26. Kwon MH et al., “The Pharmacokinetics of mRNA Vaccine Carrier using Carbon-14,” J. Radiopharm. Mol. Probes 2024, 10, 1: 73-81. doi: https://doi.org/10.22643/JRMP.2024.10.1.73
• serum, lymph nodes, muscle, spleen, liver, testis, ovary, thymus, lung, brain
27. Lehmann KJ, “SARS-CoV-2-Spike Interactions with the Renin-Angiotensin-Aldosterone System – Consequences of Adverse Reactions of Vaccination,” J Biol Today’s World 2023, 12/4: 001-013. https://doi.org/10.31219/osf.io/27g5h
• “The presented analysis provides a substantial body of evidence for the causal involvement of Ang II/activated RAAS in eliciting adverse reactions after application of spike-inducing vaccine. As an example, some serious organ disturbances or adverse reactions, in which the connection with an activated RAAS is obvious (cardiovascular and blood coagulation disorders, disorders of the nervous and muscular system, inflammatory reactions, auto-immunological, vascular and renal disorders), are presented and discussed…”
28. Li C. et al., “Intravenous Injection of Coronavirus Disease 2019 (COVID-19) MRNA Vaccine Can Induce Acute Myopericarditis in Mouse Model,” Clin. Infect. Dis. 2022, 74, 11: 1933-1950. doi: https://doi.org/10.1093/cid/ciab707
• “Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) spike antigen expression by immunostaining was occasionally found in infiltrating immune cells of the heart or injection site, in cardiomyocytes and intracardiac vascular endothelial cells, but not skeletal myocytes.”
29. Li C et al., “Mechanisms of innate and adaptive immunity to the Pfizer-BioNTech BNT162b2 vaccine,” Nature Immunol. 2022, 23: 543-555. doi: https://doi.org/10.1038/s41590-022-01163-9
• spleen, muscle, liver, lung and non-dLNs
30. Lin X et al., “Transplacental transmission of the COVID-19 vaccine messenger RNA: evidence from placental, maternal, and cord blood analyses postvaccination,” Am J Obstet Gynecol 2024, 92, 4: e13934. doi: https://doi.org/10.1111/aji.13934
• “The vaccine mRNA was detected in the 2 placentas evaluated using quantitative ddPCR and ISH… Using WES, the spike protein expression was detected in the placenta of patient 2, but not in patient 1… Furthermore, the vaccine mRNA was detected in the umbilical cord and maternal blood of patient 1 using ddPCR.”
31. Luo Y et al., “SARS-Cov-2 spike induces intestinal barrier dysfunction through the interaction between CEACAM5 and Galectin-9,” Front. Immunol. 2024, 15. doi: https://doi.org/10.3389/fimmu.2024.1303356
32. Magen E et al., “Clinical and Molecular Characterization of a Rare Case of BNT162b2 mRNA COVID-19 Vaccine-Associated Myositis,” Vaccines 2022, 10, 7: 1135. doi: https://doi.org/10.3390/vaccines10071135
• “… although the BNT162b2 vaccine mRNA was not properly expressed in blood cells seven days after receipt of the first vaccine dose, it was still expressed in muscle tissue distant from the vaccination site one month after receipt of the first vaccine dose.”
33. Magro C et al., “The histologic and molecular correlates of COVID-19 vaccine-induced changes in the skin,” Clin. Dermatol. 2021, 39, 6: 966-984. doi: https://doi.org/10.1016/j.clindermatol.2021.07.011
• Spike detected in deep dermis or blood vessels serving skin in 10/34 cases.
34. Magro C et al., “Disruption of the blood-brain barrier is correlated with spike endocytosis by ACE2 + endothelia in the CNS microvasculature in fatal COVID-19. Scientific commentary on ‘Detection of blood-brain barrier disruption in brains of patients with COVID-19, but no evidence of brain penetration by SARS-CoV-2’,” Acta Neuropathol. 2024, 147, 1: 47. doi: https://doi.org/10.1007/s00401-023-02681-y
35. Martin-Navarro L et al., “In situ detection of vaccine mRNA in the cytoplasm of hepatocytes during COVID-19 vaccine-related hepatitis,” J. Hepatol. 2023, 78, 1: e20-e22. doi: 10.1016/j.jhep.2022.08.039 https://pubmed.ncbi.nlm.nih.gov/36116717/
• “… our results suggest that lipid nanoparticles bearing mRNA molecules encoding SARS-CoV-2 proteins can reach hepatocytes under certain circumstances and deliver mRNA in high quantities that could be used by the translational machinery of the cells to produce spike.”
36. Maugeri M et al.. “Linkage between endosomal escape of LNP-mRNA and loading into EVs for transport to other cells,” Nat Commun 2019, 10: 4333.
doi: https://doi.org/10.1038/s41467-019-12275-6
• “The present study shows that LNP components (mRNA and ionizable lipids) are partly incorporated into endo-EVs… these endo-EVs protect exogenous mRNA during in vivo transport to organs…”
37. Medicines & Healthcare Products Regulatory Agency, “Summary of the Public Assessment Report for Pfizer/BioNTech COVID-19 Vaccine,” available online: https://www.gov.uk/government/publications/regulatory-approval-of-pfizer-biontech-vaccine-for-covid-19/summary-public-assessment-report-for-pfizerbiontech-covid-19-vaccine
• liver
38. Ministry of Health, Labour and Welfare of Japan, “SARS-CoV-2 mRNA Vaccine (BNT162, PF-07302048): Summary Text of the Pharmacokinetic Study,” available online: https://www.docdroid.net/xq0Z8B0/pfizer-report-japanese-government-pdf
• bladder, bone, bone marrow, brain, eyes, heart, kidneys, large intestine, liver, lung
39. Mörz M, “A Case Report: Multifocal Necrotizing Encephalitis and Myocarditis after BNT162b2 mRNA Vaccination against COVID-19,” Vaccines 2022, 10, 10: 1651. doi: https://doi.org/10.3390/vaccines10101651
• “Only spike protein but no nucleocapsid protein could be detected within the foci of inflammation in both the brain and the heart, particularly in the endothelial cells of small blood vessels.”
40. Nyein CM et al., “Severe de novo liver injury after Moderna vaccination – not always autoimmune hepatitis,” J. Hepatol. 2022, 77, 2: 556-558. Doi: 10.1016/j.jhep.2022.03.041 https://pmc.ncbi.nlm.nih.gov/articles/PMC9051901/
• “Unique to this case is the demonstration of anti-SARS-CoV-2 spike protein within the liver parenchyma.”
41. Ogata AF et al., “Circulating Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Vaccine Antigen Detected in the Plasma of mRNA-1273 Vaccine Recipients,” Clin. Infect. Dis. 2022, 75, 4: 715–718. doi: https://doi.org/10.1093/cid/ciab465
• “Here we provide evidence that circulating SARS-CoV-2 proteins are present in the plasma of participants vaccinated with the mRNA-1273 vaccine.”
42. Pateev I et al., “Biodistribution of RNA Vaccines and of Their Products: Evidence from Human and Animal Studies,” Biomedicines 2024, 12, 1: 59. doi: https://doi.org/10.3390/biomedicines12010059
• “Intravenous injection led to the detection of fluorescent proteins in the liver, spleen, lungs, and lymph nodes.”
43. Petrovszki D et al., “Penetration of the SARS-CoV-2 Spike Protein across the Blood-Brain Barrier, as Revealed by a Combination of a Human Cell Culture Model System and Optical Biosensing,” Biomedicines 2022, 10, 1: 188. doi: https://doi.org/10.3390/biomedicines10010188
44. Rhea EM et al., “The S1 protein of SARS-CoV-2 crosses the blood–brain barrier in mice,” Nature Neuroscience 2021, 24, 3: 368–378. doi: https://doi.org/10.1038/s41593-020-00771-8
45. Röltgen K et al., “Immune imprinting, breadth of variant recognition, and germinal center response in human SARS-CoV-2 infection and vaccination,” Cell, 2022, 185, 6: 1025-1040. doi: 10.1016/j.cell.2022.01.018 https://pubmed.ncbi.nlm.nih.gov/35148837/
• “mRNA vaccination stimulates robust GCs containing vaccine mRNA and spike antigen up to 8 weeks postvaccination in some cases.”
46. Rzymski P and Andrzej Fal, “To aspirate or not to aspirate? Considerations for the COVID-19 vaccines,” Pharmacol. Rep 2022, 74: 1223–1227. doi: https://doi.org/10.1007/s43440-022-00361-4
• “As shown in vivo in mice, intravenous injection of the BNT162b2 vaccine (BioNTech/Pfizer, Germany/USA) resulted in histopathological changes characteristic for myopericarditis… the amount of mRNA encoding SARS-CoV-2 spike protein and its subsequent myocardial expression was significantly higher in heart tissue when compared to the animals receiving the intramuscular injection.”
47. Sandelius A et al., “Biodistribution of lipid nanoparticle, eGFP mRNA and translated protein following subcutaneous administration in mouse,” Bioanalysis 2024, 16, 14: 721-733. doi: https://doi.org/10.1080/17576180.2024.2360361
• skin, spleen, liver, kidney
48. Sano H et al., “A case of persistent, confluent maculopapular erythema following a COVID-19 mRNA vaccination is possibly associated with the intralesional spike protein expressed by vascular endothelial cells and eccrine glands in the deep dermis,” J Dermatol 2023, 50, 9: 1208-1212. doi: https://doi.org/10.1111/1346-8138.16816
• “Surprisingly, immunohistochemical staining of the lesion 100 days after the disease onset revealed the COVID-19 spike protein expressed by vascular endothelial cells and eccrine glands in the deep dermis. As she had no episode of COVID-19 infection, it is highly likely that the spike protein was derived from the mRNA vaccine and it might be the cause of the development and persistence of her skin lesions.”
49. Sano S et al., “SARS-CoV-2 spike protein found in the acrosyringium and eccrine gland of repetitive miliaria-like lesions in a woman following mRNA vaccination,” J. Dermatol. 2024, 51, 9: e293-e295. doi: https://doi.org/10.1111/1346-8138.17204
• cutaneous
50. Sattar S Et al., “Nuclear translocation of spike mRNA and protein is a novel feature of SARS-CoV-2,” 2023 Front. Microbiol. 2023, 14 (Sec. Virology). doi: https://doi.org/10.3389/fmicb.2023.1073789
• “Although the S protein is a surface transmembrane type 1 glycoprotein, it has been predicted to be translocated into the nucleus due to the novel nuclear localization signal (NLS) “PRRARSV,” which is absent from the S protein of other coronaviruses. Indeed, S proteins translocate into the nucleus in SARS-CoV-2-infected cells. S mRNAs also translocate into the nucleus. S mRNA colocalizes with S protein, aiding the nuclear translocation of S mRNA.”
51. Schreckenberg R et al., “Cardiac side effects of RNA-based SARS-CoV-2 vaccines: Hidden cardiotoxic effects of mRNA-1273 and BNT162b2 on ventricular myocyte function and structure,” Br. J. Pharmacol. 2024, 181, 3: 345-361. doi: https://doi.org/10.1111/bph.16262
• “After 48 h, expression of the encoded spike protein was detected in ventricular cardiomyocytes for both mRNAs. At this point in time, mRNA-1273 induced arrhythmic as well as completely irregular contractions associated with irregular as well as localized calcium transients, which provide indications of significant dysfunction of the cardiac ryanodine receptor (RyR2). In contrast, BNT162b2 increased cardiomyocyte contraction via significantly increased protein kinase A (PKA) activity at the cellular level.”
52. Stern B et al., “SARS-CoV-2 spike protein induces endothelial dysfunc?on in 3D engineered vascular networks.” J. Biomed. Mater. Res. A. 2023, 112, 4: 524-533. doi: https://doi.org/10.1002/jbm.a.37543
53. Suprewicz L et al., “Blood-brain barrier function in response to SARS-CoV-2 and its spike protein,” Neurol. Neurochir Pol. 2023, 57: 14–25. doi: 10.5603/PJNNS.a2023.0014 https://pubmed.ncbi.nlm.nih.gov/36810757/
• “…the S-protein may interact directly with the BBB, and S1, S1RBD, and S2 subunits exhibit pro-inflammatory effects, resulting in increased BBB permeability via damage to tight junctions (TJs) but not adherens junctions (AJs).”
54. Suprewicz L et al., “Recombinant human plasma gelsolin reverses increased permeability of the blood-brain barrier induced by the spike protein of the SARS-CoV-2 virus,” J Neuroinflamma5on 2022, 19, 1: 282, doi: https://doi.org/10.1186/s12974-022-02642-4
55. Takanashi A et al., “Delivery and Expression of mRNA in the Secondary Lymphoid Organs Drive Immune Responses to Lipid Nanoparticle-mRNA Vaccines after Intramuscular Injection,” Mol. Pharmaceutics 2023, 20, 8: 3876–3885. doi: https://doi.org/10.1021/acs.molpharmaceut.2c01024
• “Our results suggest that the mRNA delivery and transfection of secondary lymphatic organs, not LNP adjuvancy or RNA expression in muscle, are the main drivers for adaptive immune response in mice.”
56. Yamamoto M et al., “Persistent varicella zoster virus infection following mRNA COVID-19 vaccination was associated with the presence of encoded spike protein in the lesion,” J. Cutan. Immunol. Allergy 2022, 6, 1: 18-23. doi: https://doi.org/10.1002/cia2.12278
• “Strikingly, the vaccine-encoded spike protein of the COVID-19 virus was expressed in the vesicular keratinocytes and endothelial cells in the dermis.”
57. Yonker LM et al., “Circulating Spike Protein Detected in Post–COVID-19 mRNA Vaccine Myocarditis,” Circulation 2023, 147, 11. doi: https://doi.org/10.1161/CIRCULATIONAHA.122.061025
• plasma
II. Spike protein and vaccine mRNA persistence research library
Compiled by Dr. Martin Wucher, MSC Dent Sc (eq DDS), Erik Sass, et al.
Dozens of studies collected here demonstrate that both “vaccine” mRNA, and the spike protein antigen it encodes, persist in the tissues of human vaccine recipients and animal test subjects far longer than claimed by public health officials: up to eight weeks in the case of mRNA (Röltgen K et al.) and up to six months for spike protein (Brogna C et al.). Numerous studies have also shown that viral spike proteins can persist even longer in individuals recovered from SARS CoV2 infection or with “long COVID,” with spike protein detected 15 months (Patterson BK et al.) to two years (Fraser ME at al.) after infection. Long-lasting viral spike proteins have frequently been detected in the absence of viable virus, as reflected in negative PCR tests and RNA assays, suggesting identical “vaccine” spike proteins may also persist for a year or more.
ANNOTATED REFERENCES
1. Bansal S, et al. “Cutting Edge: Circulating Exosomes with COVID Spike Protein Are Induced by BNT162b2 (Pfizer-BioNTech) Vaccination prior to Development of Antibodies: A Novel Mechanism for Immune Activation by mRNA Vaccines,” J. Immunol. 2021, 207, 10: 2405–2410. doi: https://doi.org/10.4049/jimmunol.2100637
• circulating exosomes with spike protein detected four months after vaccination.
2. Boros LG et al., “Long-lasting, biochemically modified mRNA, and its frameshifted recombinant spike proteins in human tissues and circulation after COVID-19 vaccination,” Pharmacol Res Perspect 2024, 12, 3: e1218. doi: https://doi.org/10.1002/prp2.1218
• “… clinical studies now report that modified SARS-CoV-2 mRNA routinely persist up to a month from injection and can be detected in cardiac and skeletal muscle at sites of inflammation and fibrosis, while the recombinant spike protein may persist a little over half a year in blood.”
3. Brogna C et al., “Detection of recombinant Spike protein in the blood of individuals vaccinated against SARS-CoV-2: Possible molecular mechanisms,” Proteonomics Clin App. 2023, 17, 6. doi: https://doi.org/10.1002/prca.202300048
• “The minimum and maximum time at which PP-Spike was detected after vaccination was 69 and 187 days, respectively.”
4. Castruita JAS et al., “SARS-CoV-2 spike mRNA vaccine sequences circulate in blood up to 28 days after COVID-19 vaccination,” APMIS 2023, 131: 128–132. doi: https://doi.org/10.1111/apm.13294
5. Cheung CCL et al., “Residual SARS-CoV-2 viral antigens detected in GI and hepatic tissues from five recovered patients with COVID-19,” Gut 2022, 71, 1: 226–9. doi: https://doi.org/10.1136/gutjnl-2021-324280
• Persistence of residual SARS-CoV-2 antigens up to 180 days in the colon, appendix, ileum, haemorrhoid, liver, gallbladder and lymph nodes; unable to detect viral RNA in many patients’ tissues.
6. Colmenero I et al., “SARS-CoV-2 endothelial infection causes COVID-19 chilblains: histopathological, immunohistochemical and ultrastructural study of seven paediatric cases,” Br J Dermatol. 2020, 183: 729-737. doi: https://doi.org/10.1111/bjd.19327
• Spike protein detected in lesions up to 30 days after onset of acute infection. SARS-CoV-2 PCR from nasopharyngeal and oropharyngeal swabs was negative in all cases tested (six of six).
7. Craddock V et al., “Persistent circulation of soluble and extracellular vesicle-linked Spike protein in individuals with postacute sequelae of COVID-19,” J Med. Virol. 2023, 95, 2: e28568. doi: https://doi.org/10.1002/jmv.28568
• “… our findings suggest that Spike and/or viral RNA fragments persist in the recovered COVID-19 patients with PASC up to 1 year or longer after acute SARS-CoV-2 infection.” Further, “this is the first report to show that part of the circulating Spike is linked to extracellular vesicles without any presence of viral RNA in these vesicles.”
8. European Medicines Agency, Assessment Report, available online: https://www.ema.europa.eu/en/documents/assessment-report/comirnaty-epar-public-assessment-report_en.pdf
• “Synthetic mRNAs encapsulated in LNPs can reach many organs, such as the spleen, heart, kidneys, lungs and brain. The mRNAs were found in the ovaries and the testicles in small quantities, during the biodistribution studies of this vaccine after 9 days…”
9. Fertig TE et al., “Vaccine mRNA Can Be Detected in Blood at 15 Days Post Vaccination,” Biomedicines 2022, 10, 7: 1538. doi: https://doi.org/10.3390/biomedicines10071538
10. Fraser ME at al., “SARS-CoV-2 Spike Protein and Viral RNA Persist in the Lung of Patients With Post-COVID Lung Disease (abstract),” Am J Respir Crit Care Med 2024, 209: A4193. doi: https://doi.org/10.1164/ajrccm-conference.2024.209.1_MeetingAbstracts.A4193
• “Spike protein and RNA persists in BAL from patients with post-COVID lung disease up to two years after acute infection.”
11. Gaebler C et al., “Evolution of antibody immunity to SARS-CoV-2,” Nature 2021, 591: 639-644. doi: https://doi.org/10.1038/s41586-021-03207-w
• Gastrointestinal tract biopsies suggest spike antigen persisted in the small bowel in 7 of 14 individuals who were asymptomatic at 4 months after infection… Clinically approved nasopharyngeal-swab PCR assays were negative in all 14 individuals at the time of biopsy. However, biopsy samples from 3 of the 14 participants produced PCR amplicons that were sequence-verified as SARS-CoV-2. In addition, viral RNA was detected by in situ hybridization in biopsy samples from the two participants who were tested.
12. George S et al., “Evidence for SARS-CoV-2 Spike Protein in the Urine of COVID-19 Patients,” Kidney360 2021, 2, 6: 924-936. doi: 10.34067/KID.0002172021 https://pubmed.ncbi.nlm.nih.gov/35373072/
• “The SARS-CoV-2 spike protein could be detected in urine from day 1 to day 44 post–hospital admission… Of the 23 adults who were Ur-S+, only one individual showed detectable viral RNA in urine.”
13. Goh D et al., “Case report: Persistence of residual antigen and RNA of the SARS-CoV-2 virus in tissues of two patients with long COVID,” Front. Immunol. 2022, 13 (Sec. Viral Immunology). doi: https://doi.org/10.3389/fimmu.2022.939989
• Persistence of spike protein 426 days after symptom onset; residual viral RNA also detected.
14. Hano S et al., “A case of persistent, confluent maculopapular erythema following a COVID-19 mRNA vaccination is possibly associated with the intralesional spike protein expressed by vascular endothelial cells and eccrine glands in the deep dermis,” J Dermatol 2023, 50, 9: 1208-1212. doi: https://doi.org/10.1111/1346-8138.16816
• “Surprisingly, immunohistochemical staining of the lesion 100 days after the disease onset revealed the COVID-19 spike protein expressed by vascular endothelial cells and eccrine glands in the deep dermis. As she had no episode of COVID-19 infection, it is highly likely that the spike protein was derived from the mRNA vaccine and it might be the cause of the development and persistence of her skin lesions.”
15. Karaba AH et al., “Detectable plasma severe acute respiratory syndrome coronavirus 2 spike antigen is associated with poor antibody response following third messenger RNA vaccination in kidney transplant recipients,” Transpl Infect Dis 2024, 26, 3: e14281. doi: https://doi.org/10.1111/tid.14281
• Spike protein detectable in 3/16 (19%) participants 14 days after vaccination.
16. Kawano H et al., “Fulminant Myocarditis 24 Days after Coronavirus Disease Messenger Ribonucleic Acid Vaccination,” Intern. Med. 2022, 61, 15: 2319-2325. doi: https://doi.org/10.2169/internalmedicine.9800-22
• “… positive immunostaining for severe acute respiratory syndrome coronavirus 2 spike protein and C4d in the myocardium."
17. Kent SJ et al., “Blood Distribution of SARS-CoV-2 Lipid Nanoparticle mRNA Vaccine in Humans,” ACS Nano 2024, 18, 39: 27077-27089. doi: https://doi.org/10.1021/acsnano.4c11652
• “The vaccine mRNA was detectable and quantifiable up to 14–15 days postvaccination in 37% of subjects.”
18. Krauson AM et al., “Duration of SARS-CoV-2 mRNA vaccine persistence and factors associated with cardiac involvement in recently vaccinated patients,” npj Vaccines, 8, 141. doi: https://doi.org/10.1038/s41541-023-00742-7
• “Vaccine was detected in the axillary lymph nodes in the majority of patients dying within 30 days of vaccination… Vaccine was detected in the myocardium in a subset of patients vaccinated within 30 days of death.”
19. Li C et al., “Mechanisms of innate and adaptive immunity to the Pfizer-BioNTech BNT162b2 vaccine,” Nature Immunol. 2022, 23: 543-555.
doi: https://doi.org/10.1038/s41590-022-01163-9
• “mRNA could be detected in the spleen, and the spike protein itself was detectable in the serum, for up to 7 d after immunization.”
20. Magen E et al., “Clinical and Molecular Characterization of a Rare Case of BNT162b2 mRNA COVID-19 Vaccine-Associated Myositis,” Vaccines 2022, 10, 7: 1135. doi: https://doi.org/10.3390/vaccines10071135
• “… although the BNT162b2 vaccine mRNA was not properly expressed in blood cells seven days after receipt of the first vaccine dose, it was still expressed in muscle tissue distant from the vaccination site one month after receipt of the first vaccine dose.”
21. Mayordomo-Colunga J et al., “SARS-CoV-2 spike protein in intestinal cells of a patient with coronavirus disease 2019 multisystem inflammatory syndrome,” J Pediatr. 2022, 243: 214-18e215. doi: https://doi.org/10.1016/j.jpeds.2021.11.058
• Spike protein detected 6 weeks after acute infection. “At presentation, the patient tested negative for SARS-CoV-2 by reverse-transcriptase polymerase chain reaction on nasopharyngeal swab but positive for serum SARS-CoV-2 immunoglobulin G.”
22. Mörz M, “A Case Report: Multifocal Necrotizing Encephalitis and Myocarditis after BNT162b2 mRNA Vaccination against COVID-19,” Vaccines 2022, 10, 10: 1651. doi: https://doi.org/10.3390/vaccines10101651
• Vaccine-induced spike detected on autopsy three weeks after last injection.
23. Ogata AF et al., “Circulating Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Vaccine Antigen Detected in the Plasma of mRNA-1273 Vaccine Recipients,” Clin. Infect. Dis. 2022, 74, 4: 715-728. doi: https://doi.org/10.1093/cid/ciab465
• “Spike protein was detectable in 3 of 13 participants an average of 15 days after the first injection.”
24. Parcial ALN et al., “SARS-CoV-2 Is Persistent in Placenta and Causes Macroscopic, Histopathological, and Ultrastructural Changes,” Viruses 2022, 14, 9: 1885. doi: https://doi.org/10.3390/v14091885
• “Three of five placentas presented SARS-CoV-2 RNA detected by RT-PCRq at least two to twenty weeks after primary pregnancy infection symptoms, and SARS-CoV-2 spike protein was detected in all placentas by immunoperoxidase assay.”
25. Pateev I et al., “Biodistribution of RNA Vaccines and of Their Products: Evidence from Human and Animal Studies,” Biomedicines 2024, 12, 1: 59. doi: https://doi.org/10.3390/biomedicines12010059
• (Roltgen K et al) “The amount of the spike antigen declined significantly at 4 months after the double vaccination but was still detectable.”
• “Immunohistochemical staining for the spike antigen in the lymph nodes of vaccinated patients revealed peak amounts of the spike protein in germinal centers 16 days after dose 2, with the spike antigen still detectable on day 60.”
• (Brogna C et al.) “It is noteworthy that in this study, spike protein was still detected in human blood on the 187th day after vaccination.”
26. Patterson BK et al., “Persistence of SARS CoV-2 S1 Protein in CD16+ Monocytes in Post-Acute Sequelae of COVID-19 (PASC) up to 15 Months Post-Infection,” Front. Immunol. 2022, 12: 746021. doi: https://doi.org/10.3389/fimmu.2021.746021
• Intact viral RNA undetectable in monocytes.
27. Peluso MJ et al., “Plasma-based antigen persistence in the post-acute phase of COVID-19,” Lancet 2024, 24, 6: E345-E347. doi: 10.1016/S1473-3099(24)00211-1 https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(24)00211-1/fulltext
• “Of 660 pandemic-era specimens tested, 61 (9·2%) specimens from 42 participants (25% of the group), had one or more detectable SARS-CoV-2 antigens. The most commonly detected antigen was spike (n=33, 5·0%), followed by S1 (n=15, 2·3%)…”
• “… our data provide strong evidence that SARS-CoV-2, in some form or location, persists for up to 14 months following acute SARS-CoV-2 infection.”
• “… our findings provide no direct evidence regarding the persistent presence of replication-competent or even transcriptionally active virus.”
28. Peluso MJ et al., “SARS-CoV-2 and mitochondrial proteins in neural-derived exosomes of COVID-19,” Ann Neurol 2022, 91, 6: 772-781. doi: https://doi.org/10.1002/ana.26350
• Exosomes containing spike protein were detected in plasma of long COVID patients with neuropsychiatric symptoms at two months.
29. Roden AC et al., “Comparison of In Situ Hybridization, Immunohistochemistry, and Reverse Transcription–Droplet Digital Polymerase Chain Reaction for Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Testing in Tissue,” Arch Pathol Lab Med 2021, 145, 7: 785–796. doi: https://doi.org/10.5858/arpa.2021-0008-SA
• Detected viral protein 46 days after onset of symptoms.
• “All patients from our institution had tested positive for COVID-19 by nasopharyngeal swab within a median of 14.5 days (range, 0–67 days) before death. All patients from our institution but one were tested for COVID-19 again at time of autopsy; 10 of 13 (76.9%) tested positive.”
30. Röltgen K et al., “Immune imprinting, breadth of variant recognition, and germinal center response in human SARS-CoV-2 infection and vaccination,” Cell, 2022, 185, 6: 1025-1040. doi: 10.1016/j.cell.2022.01.018 https://pubmed.ncbi.nlm.nih.gov/35148837/
• “mRNA vaccination stimulates robust GCs containing vaccine mRNA and spike antigen up to 8 weeks postvaccination in some cases.”
• “… with spike antigen still present as late as 60 days post-second dose”
31. Rong Z et al., “Persistence of spike protein at the skull-meninges-brain axis may contribute to the neurological sequelae of COVID-19,” Cell Host Microbe 2024, 26: S1931-3128(24)00438-4. doi: 10.1016/j.chom.2024.11.007 https://pubmed.ncbi.nlm.nih.gov/39615487/
• “In a time course experiment, we found the spike protein in the skull marrow, kidney, liver, and lung 3 days post-injection, remaining detectable in the kidney and liver 14 days post-injection.”
32. Sano H et al., “A case of persistent, confluent maculopapular erythema following a COVID-19 mRNA vaccination is possibly associated with the intralesional spike protein expressed by vascular endothelial cells and eccrine glands in the deep dermis,” J. Dermatol. 2023, 50: 1208–1212. doi: https://doi.org/10.1111/1346-8138.16816
• “Surprisingly, immunohistochemical staining of the lesion 100 days after the disease onset revealed the COVID-19 spike protein expressed by vascular endothelial cells and eccrine glands in the deep dermis. As she had no episode of COVID-19 infection, it is highly likely that the spike protein was derived from the mRNA vaccine and it might be the cause of the development and persistence of her skin lesions.”
33. Schultheiss C et al., “Liquid biomarkers of macrophage dysregulation and circulating spike protein illustrate the biological heterogeneity in patients with post-acute sequelae of COVID-19,” J Med Virol 2023, 95, 1: e28364. doi: https://doi.org/10.1002/jmv.28364
• Detected SARS-CoV-2 S1 protein in the plasma of approximately 64% of PASC study participants recruited at a median of 8 months (range 1–17 months) after acute COVID-19, but only in approximately 35% of convalescent control patients.
34. Swank Z et al., “Persistent circulating SARS-CoV-2 spike is associated with post-acute COVID-19 sequelae,” Clin. Infect. Dis. 2022, 76: e487-e490. doi: https://doi.org/10.1093/cid/ciac722
• “We detect severe acute respiratory syndrome coronavirus 2 spike predominantly in PASC patients up to 12 months after diagnosis… Although the detection of spike in PASC patients months after diagnosis suggests the presence of replicating viral reservoirs, further analyses are needed to confirm this hypothesis.”
35. Visvabharathy L et al., “Case report: Treatment of long COVID with a SARS-CoV-2 antiviral and IL-6 blockade in a patient with rheumatoid arthritis and SARS-CoV-2 antigen persistence,” Front. Med. 2022, 9 (Sec. Infectious Diseases – Surveillance). doi: https://doi.org/10.3389/fmed.2022.1003103
• “The patient tested RT-PCR– for SARS-CoV-2 at 14 days post-infection and multiple times thereafter but continued to test intermittently antigen+ for 14 weeks post-infection despite no overt exposure to SARS-CoV-2 infected individuals.”
36. Wu H et al., “Molecular evidence suggesting the persistence of residual SARS-CoV-2 and immune responses in the placentas of pregnant patients recovered from COVID-19,” Cell Prolif. 2021, 54, 9:e13091. doi: https://doi.org/10.1111/cpr.13091
• “Our study showed that SARS-CoV-2 nucleic acid (in one patient) and protein (in five patients) were present in the placentas of clinically recovered pregnant patients for more than 3 months after diagnosis.”
37. Yamamoto M et al., “Persistent varicella zoster virus infection following mRNA COVID-19 vaccination was associated with the presence of encoded spike protein in the lesion,” J. Cutan. Immunol. Allergy 2022, 6, 1: 18-23. doi: https://doi.org/10.1002/cia2.12278
• “multi-dermatomal vesicles, necrotizing vasculitis and superficial thrombophlebitis-like lesions, which lasted as long as 3 months possibly associated with two doses of BNT162b2”
38. Yonker LM et al., “Multisystem inflammatory syndrome in children is driven by zonulin-dependent loss of gut mucosal barrier,” J Clin Invest. 2021, 131, 14: e149633. doi: https://doi.org/10.1172/JCI149633
• “…our studies showed that spike antigens rose over the first few days of MIS-C symptoms and persisted for more than 10 days, occasionally through 6 months…”
• “… we measured SARS-CoV-2 RNA from MIS-C stool samples collected several weeks after the initial SARS-CoV-2 infection or exposure. Indeed, a majority of the patients showed detectable viral loads in the stool ranging from 1.5 × 102 to 2.5 × 107 RNA copies/mL, suggesting an ongoing nidus of infection in MIS-C.”
39. Zollner A et al., “Postacute COVID-19 is Characterized by Gut Viral Antigen Persistence in Inflammatory Bowel Diseases,” Gastroenterology 2022, 163, 2: 495-506.e8. doi: https://doi.org/10.1053/j.gastro.2022.04.037
• Viral spike protein detected 219 days after original positive endoscopy in gut lining of 15 out of 132 subjects.
• “We were unable to culture SARS-CoV-2 from gut tissue of patients with viral antigen persistence.”
III. Lipid nanoparticle toxicity and allergenicity research library
Compiled by Dr. Byram Bridle, PhD, Erik Sass, et al.
The anti-SARS CoV2 mRNA injections rely on lipid nanoparticles (LNPs) bonded with polyethylene glycol (PEG) to deliver mRNA coding for the spike protein antigen into human cells. However, a growing body of evidence suggests that the ionizable LNPs used in the experimental mRNA injections are highly inflammatory on their own, while PEG has long been recognized as an allergen with the potential to trigger anaphylaxis (a severe, possibly life-threatening allergic reaction). This annotated research collection presents over 50 scientific papers detailing the potential harms of LNPs, PEG, and other components of the mRNA injections to the human body and setting forth possible or established mechanisms. Some of the research annotated here also suggests a far higher incidence of anaphylaxis due to the mRNA injections than claimed in official estimates, ranging from 1/2,280 doses (Warren CM et al.) to 1/4,049 (Blumenthal KG et al.) and 1/13,882 (Somiya A et al.).
ANNOTATED REFERENCES
1. Ahn JH et al., “Impact of administration routes and dose frequency on the toxicology of SARS-CoV-2 mRNA vaccines in mice model,” Arch Toxicol. 2024. doi: https://doi.org/10.1007/s00204-024-03912-1
• “These results suggest that mRNA vaccines may exhibit various potential toxicities, and the toxicological phenotype may vary depending on the LNP composition.”
2. Awaya T et al., “Cytokine Storms and Anaphylaxis Following COVID-19 mRNA-LNP Vaccination: Mechanisms and Therapeutic Approaches,” Diseases 2024, 12, 10: 231. doi: https://doi.org/10.3390/diseases12100231
• “…during the process of endosomal escape, ionizable lipids disrupt the endosomal membrane to release mRNA, which can, in some cases, lead to the excessive production of inflammatory cytokines.”
3. Bakos T et al., “mRNA-LNP COVID-19 Vaccine Lipids Induce Complement Activation and Production of Proinflammatory Cytokines: Mechanisms, Effects of Complement Inhibitors, and Relevance to Adverse Reactions,” Int. J. Mol. Sci. 2024, 25, 7: 3595. doi: https://doi.org/10.3390/ijms25073595
• “… the novel findings in the present study include (i) the dominance of alternative pathway activation, (ii) the increased strength of C activation relative to corresponding PEGylated liposomes, and (iii) the absence of C activation by naked mRNAs.”
4. Barta BA et al., “The COVID-19 mRNA vaccine Comirnaty induces anaphylactic shock in an anti-PEG hyperimmune large animal model,” Eur. Heart J. 2023, 44 (supp 2): ehad655.3291. doi: https://doi.org/10.1093/eurheartj/ehad655.3291
• “Consistent with previous studies, our current data show a causal role of anti-PEG Abs in the anaphylaxis to Comirnaty, which involves complement activation…”
5. Bitounis D et al., “Strategies to reduce the risks of mRNA drug and vaccine toxicity,” Nat. Rev. Drug Discov. 2024, 23: 281-300. doi: https://doi.org/10.1038/s41573-023-00859-3
• “… cell tropism and tissue distribution of mRNA and lipid nanoparticles can lead to toxicity, and their possible reactogenicity.”
6. Blumental KG et al., “Acute Allergic Reactions to mRNA COVID-19 Vaccines,” JAMA 2021, 325, 15:1562-1565. Doi: 10.1001/jama.2021.3976 https://jamanetwork.com/journals/jama/fullarticle/2777417
• “… severe reactions consistent with anaphylaxis occurred at a rate of 2.47 per 10 000 vaccinations… The incidence rate of confirmed anaphylaxis in this study is larger than that reported by the Centers for Disease Control and Prevention based on passive spontaneous reporting methods (0.025-0.11 per 10 000 vaccinations).”
7. Cabanillas B et al., “Allergic reactions to the first COVID-19 vaccine: A potential role of polyethylene glycol?” Allergy 2021, 76, 6: 1617-1618. doi: https://doi.org/10.1111/all.14711
• “Although the trigger of the adverse allergic reactions suffered by the two NHS workers after receiving the vaccine BNT162b2 against COVID-19 has yet to be determined, the potential role of the excipient ALC-0159 containing PEG as a high-risk hidden trigger of dangerous allergic reactions should be carefully considered before advising the administration of BNT162b2 vaccine.”
8. Calogiuri G et al., “Polyethylene glycols and polysorbates: Two still neglected ingredients causing true IgE-mediated reactions,” J Allergy Clin Immunol Pract 2019, 7, 7: 2509-2510. doi:10.1016/j.jaip.2019.05.058 https://www.jaci-inpractice.org/article/S2213-2198(19)30591-4/fulltext
• “In the light of increased exposure of PEGs and polysorbates in our environment, a greater incidence of PEG hypersensitivity should be expected in the next years.”
9. Camera GL et al., “A Step-by-Step Approach to Improve Clinical Translation of Liposome-Based Nanomaterials, a Focus on Innate Immune and Inflammatory Responses,” Int. J. Mol. Sci. 2021, 22, 2: 820. doi: https://doi.org/10.3390/ijms22020820
• “… a large proportion of the selected, commercially available carriers failed to pass the first homogeneity tests, and further products were found to be cytotoxic or interact with the immune system in an undesired way.”
10. Carreno JM et al., “mRNA-1273 but not BNT162b2 induces antibodies against polyethylene glycol (PEG) contained in mRNA-based vaccine formulations,” Vaccine 2022, 40, 42: 6114-6124. doi: https://doi.org/10.1016/j.vaccine.2022.08.024
• “We detected an increase in the reactivity to mRNA vaccine formulations in mRNA-1273 but not BNT162b2 vaccinees’ sera in a prime-boost dependent manner. Furthermore, we observed the same pattern of reactivity against irrelevant lipid nanoparticles.”
11. Catenacci L et al., “Effect of Lipid Nanoparticle Physico-Chemical Properties and Composition on Their Interaction with the Immune System,” Pharmaceutics 2024, 16, 12: 1521. doi: https://doi.org/10.3390/pharmaceutics16121521
• “COVID-19 mRNA vaccines administered in the deltoid muscle in humans stimulate inflammation and recruitment of neutrophils, monocytes, and dendritic cells...”
12. Chen BM et al., “Polyethylene Glycol Immunogenicity: Theoretical, Clinical, and Practical Aspects of Anti-Polyethylene Glycol Antibodies,” ACS Nano 2021, 15, 9: 14022–14048. doi: https://doi.org/10.1021/acsnano.1c05922
• “Hypersensitivity reactions including anaphylaxis after infusion of pegylated medicines are well documented in both animal and clinical studies… Pegylated liposomes encapsulating oligonucleotides induce anti-PEG IgM antibodies in mice and cause anaphylactic shock upon a second injection of liposomes.”
13. Chen WA et al., “Antibodies against Poly(ethylene glycol) Activate Innate Immune Cells and Induce Hypersensitivity Reactions to PEGylated Nanomedicines,” ACS Nano 2023, 17, 6: 5757–5772. doi: https://doi.org/10.1021/acsnano.2c12193
• “We demonstrate that anti-PEG IgG but not IgM antibodies induce hypersensitivity-like symptoms against PLD and other PEGylated nanoparticles and macromolecules in mice that depend primarily on neutrophils, macrophages, and basophils.”
14. de Vriez J, “Pfizer's vaccine raises allergy concerns. Polymer in mRNA's “packaging” may cause rare anaphylactic reactions,” Science 2021, 371, 6524: 10-11. doi: 10.1126/science.371.6524.10 https://www.science.org/doi/10.1126/science.371.6524.10
• “Severe allergy-like reactions in at least 12 people who received the COVID-19 vaccine produced by Pfizer and BioNTech may be due to a compound in the packaging of the messenger RNA (mRNA) that forms the vaccine's main ingredient, scientists say. A similar mRNA vaccine developed by Moderna also contains the compound, polyethylene glycol (PEG).”
15. du Preez HN et al., “COVID-19 vaccine adverse events: Evaluating the pathophysiology with an emphasis on sulfur metabolism and endotheliopathy,” Eur J Clin Invest. 2024, 54, 10: e14296. doi: https://doi.org/10.1111/eci.14296
• “We hypothesize that after COVID-19 vaccination, the combination of the genetic-vaccine- generated (GVG) Sp antigen, the genetic material and LNPs, will ultimately contribute to GL [glycocalyx] degradation; mainly through the generation of chronic, skewed or excessive inflammatory responses, and oxidative stress. Therefore, AEs experienced postvaccination results from compromised barrier functions, circulating pro-inflammatory cytokines, reactive oxygen species (ROS), GL fragments, harmful NPs, and soluble GVG Sp and its fragments, all of which cause various cytotoxic effects.”
16. Gao Z et al., “Exploring the impact of lipid nanoparticles on protein stability and cellular proteostasis,” J. Colloid Interface Sci. 2025, 678(A): 656-665. doi: https://doi.org/10.1016/j.jcis.2024.08.146
• “… LNPs may induce subtle proteome stress by compromising protein stability and proteostasis even without obvious damage to cell viability.”
17. Guo C et al., “The interplay between PEGylated nanoparticles and blood immune system,” Adv Drug Deliv Rev. 2023, 200: 114004. doi: https://doi.org/10.1016/j.addr.2023.115044
• “Complement activation-related pseudoallergy (CARPA) and accelerated blood clearance (ABC) phenomenon are the most notorious problems. CARPA is a non-IgE-activated hypersensitivity reaction (HSR) that manifests as a hemodynamic disturbance and an inflammatory response that can cause serious consequences or even fatalities.”
18. Ibrahim M et al., “Polyethylene glycol (PEG): The nature, immunogenicity, and role in the hypersensitivity of PEGylated products,” J Control Release 2022, 351: 215-230. doi: https://doi.org/10.1016/j.jconrel.2022.09.031
• “… the main causes and exact mechanisms of hypersensitivity to mRNA COVID-19 vaccines have not been fully elucidated, but reports of hypersensitivity reactions have focused on the role of the PEG polymer that is used in the preparation of these vaccines… we explain the potential role of PEG in the reports of the immunogenicity and hypersensitivity that has been encountered post-mRNA COVID-19 vaccination.”
19. Igyarto BZ et al., “Future considerations for the mRNA-lipid nanoparticle vaccine platform,” Curr Opin Virol. 2021, 48: 65–72. doi: 10.1016/j.coviro.2021.03.008 https://pubmed.ncbi.nlm.nih.gov/33906124/
• “… some of the immediate allergic responses observed with the first shot of mRNA-LNP vaccines might be related to pre-existing PEG antibodies. Since these vaccines often require a booster shot, anti-PEG antibody formation is expected after the first shot. Thus, the allergic events are likely to increase upon re-vaccination.”
• “It has been shown that mRNA-LNP vaccines have an altered tissue distribution, dynamics, and uptake in animals that have been pre-exposed to inflammatory agents. These findings suggest that people with pre-existing inflammatory conditions might show altered immune responses to these vaccines and might present with more severe side-effects.”
20. Igyarto BZ and Zhen Qin, “The mRNA-LNP vaccines – the good, the bad and the ugly?” Front. Immunol. 2024, 15 (Sec. Vaccines and Molecular Therapeutics). doi: https://doi.org/10.3389/fimmu.2024.1336906
• “… the LNPs’ ionizable lipid component of the mRNA-LNP vaccine is highly inflammatory … another potential explanation for the distinct lots triggering different levels of adverse events could be that the amounts of mRNA-LNP or the mRNA : LNP ratio differed between lots.”
21. Ju Y et al., “Anti-PEG Antibodies Boosted in Humans by SARS-CoV-2 Lipid Nanoparticle mRNA Vaccine,” ACS Nano 2022, 16, 8: 11769–11780. doi: https://doi.org/10.1021/acsnano.2c04543
• “We conclude that PEG-specific antibodies can be boosted by LNP mRNA vaccination and that the rise in PEG-specific antibodies is associated with systemic reactogenicity and an increase of PEG particle–leukocyte association in human blood.”
22. Klimek L et al., “Allergenic components of the mRNA-1273 vaccine for COVID-19: Possible involvement of polyethylene glycol and IgG-mediated complement activation,” Allergy 2021, 76, 11: 3307-3313. doi: https://doi.org/10.1111/all.14794
• “Allergic reactions to such PEGylated lipids are IgE-mediated. However, non-IgE-mediated reactions should also be considered.”
23. Korzun T et al., “From Bench to Bedside: Implications of Lipid Nanoparticle Carrier Reactogenicity for Advancing Nucleic Acid Therapeutics,” Pharmaceuticals 2023, 16, 8: 1088. doi: https://doi.org/10.3390/ph16081088
• “… the current data raise important questions revolving around LNP-associated side effects. For instance, the use of a greater mRNA–LNP dose in the mRNA-1273 vaccine and different ionizable lipids used in the formulation are potential explanations for the increased reactogenicity of mRNA-1273 compared with BNT162b formulations in the Moderna and Pfizer-BioNTech COVID- 19 vaccines, respectively.”
24. Korzun T et al., “Lipid Nanoparticles Elicit Reactogenicity and Sickness Behavior in Mice Via Toll-Like Receptor 4 and Myeloid Differentiation Protein 88 Axis,” ACS Nano 2024, 18, 36: 24842–24859. doi: https://doi.org/10.1021/acsnano.4c05088
• “Our comprehensive investigation utilizing gene ablation studies and pharmacological receptor manipulation proves that TLR4 activation by LNPs triggers distinct physiologically meaningful responses in mice. We show that TLR4 and MyD88 are essential for reactogenic signal initiation, pro-inflammatory gene expression, and physiological outcomes like food intake and body weight ─ robust metrics of sickness behavior in mice.”
25. Kozma GT et al., “Anti-PEG antibodies: Properties, formation, testing and role in adverse immune reactions to PEGylated nano-biopharmaceuticals,” Adv. Drug Deliv. Rev. 2020, 154-155: 163-175. doi: https://doi.org/10.1016/j.addr.2020.07.024
• “Considering the known causal relationships among C [complement] activation, ABC [accelerated blood clearance], HSRs [hypersensitivity reactions], opsonization and immunogenicity, we proposed the possible rise of an immune stimulatory vicious cycle among these effects…”
26. Kozma GT et al., “Role of anti-polyethylene glycol (PEG) antibodies in the allergic reactions to PEG-containing Covid-19 vaccines: Evidence for immunogenicity of PEG,” Vaccine 2023, 41, 31: 4561-4570. doi: https://doi.org/10.1016/j.vaccine.2023.06.009
• “The anti-PEG IgG and/or IgM levels in the 15 vaccine reactors (3 anaphylaxis) were significantly higher compared to nonreactors. Serial testing of plasma showed significant correlation between the booster injection-induced rises of anti-S and anti-PEG IgGs, suggesting coupled anti-S and anti-PEG immunogenicity.”
27. Luxi N et al., “Allergic Reactions to COVID-19 Vaccines: Risk Factors, Frequency, Mechanisms and Management,” BioDrugs 2022, 36: 443-458. doi: https://doi.org/10.1007/s40259-022-00536-8
• “PEG is the only excipient in COVID-19 vaccines that has been clearly demonstrated to cause mainly immediate HRs, while the role of trometamol and PS80 as relevant allergens in these vaccines remains more questionable.”
28. Maltezou HC et al., “Anaphylaxis rates following mRNA COVID-19 vaccination in children and adolescents: Analysis of data reported to EudraVigilance,” Vaccine 2023, 41, 14: 2382-2386. doi: https://doi.org/10.1016/j.vaccine.2023.02.067
• “The overall mean anaphylaxis rate was 12.81 [95% confidence interval (CI): 11.49–14.12] per 106 mRNA vaccine doses [12.14 (95% CI: 6.37–17.91) per 106 doses for mRNA-1273 and 12.84 (95% CI: 11.49–14.19) per 106 doses for BNT162b2].”
29. Maugeri M et al.. “Linkage between endosomal escape of LNP-mRNA and loading into EVs for transport to other cells,” Nat Commun 2019, 10: 4333. doi: https://doi.org/10.1038/s41467-019-12275-6
• “… the systemic delivery of both EVs and LNPs cause the expression of proinflammatory cytokines in mice…”
30. Moghimi SM, “Allergic reactions and anaphylaxis to LNP-based COVID-19 vaccines,” Mol. Ther. 2021, 29, 3: 898-900. doi: 10.1016/j.ymthe.2021.01.030 https://pubmed.ncbi.nlm.nih.gov/33571463
• “Limited information is available on LNP size distribution, polydispersity index, particle number,and presence of likely co-existing vesicles and micelles in the Pfizer-BioNTech and Moderna vaccines. Batch-to-batch variations in these parameters could further play a modulatory role in allergic reactions, and these possibilities were previously suggested for liposomes.”
31. Moghimi SM and Dmitri Simberg, “Pro-inflammatory concerns with lipid nanoparticles,” Mo. Ther. 2022, 30, 6: 2109-2110. doi: 10.1016/j.ymthe.2022.04.011 https://pubmed.ncbi.nlm.nih.gov/35487214/
• “Considering the pro-inflammatory nature of the currently available ionizable cationic lipids, notably their undesirable immune cascade initiated through the IL-1β release, and of other cationic lipids, the potential application of LNPs for systemic administration must be viewed cautiously.”
32. Mouri M et al., “Serum polyethylene glycol-specific IgE and IgG in patients with hypersensitivity to COVID-19 mRNA vaccines,” Allergol Int. 2022, 71, 4: 512-519. doi: https://doi.org/10.1016/j.alit.2022.05.007
• “The results suggest that PEG is one of the antigens in the allergy to COVID-19 mRNA vaccines. Cross-reactivity between PEG and PS might be crucial for allergy to the vaccines.”
33. Nakayama T et al., “Comparison of cytokine production in mice inoculated with messenger RNA vaccines BNT162b2 and mRNA-1273,” Microbiol Immunol 2022, 67, 3: 120-128. doi: https://doi.org/10.1111/1348-0421.13043
• “The induction of inflammatory cytokines in the mouse model is related to the cause of adverse events in humans, with a higher incidence of adverse events after the second dose.”
34. Ndeupen S et al., “The mRNA-LNP platform's lipid nanoparticle component used in preclinical vaccine studies is highly inflammatory,” iScience 2021, 24, 12: 103479. doi: 10.1016/j.isci.2021.103479 https://pubmed.ncbi.nlm.nih.gov/34841223/
• “Intradermal injection of these LNPs alone or in combination with non-coding poly-cytosine mRNA led to rapid and robust innate inflammatory responses, characterized by neutrophil infiltration, activation of diverse inflammatory pathways, and production of various inflammatory cytokines and chemokines. The same dose of LNP delivered intranasally led to similar inflammatory responses in the lung and resulted in a high mortality rate.”
35. Parhiz H et al., “Added to pre-existing inflammation, mRNA-lipid nanoparticles induce inflammation exacerbation (IE),” J Control Release 2022, 344: 50-61. doi: https://doi.org/10.1016/j.jconrel.2021.12.027
• “Although fairly benign in the healthy state, LNP potentiated existing inflammation in mice that had received the bacterial cell wall component LPS intratracheally (IT) or intravenously (IV).”
36. Qin Z et al., “Pre-exposure to mRNA-LNP inhibits adaptive immune responses and alters innate immune fitness in an inheritable fashion,” PLoS Pathog. 2022, doi: https://doi.org/10.1371/journal.ppat.1010830
• “The mRNA-LNP-based SARS-CoV-2 vaccine is highly inflammatory, and its synthetic ionizable lipid component responsible for the induction of inflammation has a long in vivo half-life… We found that pre-exposure to mRNA-LNPs or LNP alone led to long-term inhibition of the adaptive immune response.”
37. Radice A et al., “Potential culprits for immediate hypersensitivity reactions to BNT162b2 mRNA COVID-19 vaccine: not just PEG,” Eur Ann Allergy Clin Immunol 2021, 53, 5: 240-242. doi: https://doi.org/10.23822/eurannaci.1764-1489.214
• “Apart from PEG, another component of the LNP, 1,2-distearoyl-sn-glycero-3-phosphocholine (DSPC), should also be considered a potential culprit as it contains a quaternary ammonium (QA) ion.”
38. Rama TA et al., “Hypersensitivity to the Moderna COVID-19 vaccine caused by tromethamine: PEG is not always the culprit excipient,” J Investig Allergol Clin Immunol. 2022, 32, 5: 414-415. doi: 10.18176/jiaci.0773
https://www.jiaci.org/revistas/doi10.18176_jiaci.0773.pdf
• “… this case provides further evidence that the excipient, and specifically IgE-mediated hypersensitivity to tromethamine, may be an underlying mechanism for immediate hypersensitivity to mRNA COVID-19 vaccines.”
39. Sampath V et al., “Vaccines and allergic reactions: The past, the current COVID-19 pandemic, and future perspectives,” Allergy 2021, 76, 6: 1640-1660. doi: https://doi.org/10.1111/all.14840
• “This suggests that the incidence of anaphylaxis in the mRNA BNT162b2 (11.1 cases per million doses) and mRNA-1273 COVID-19 vaccines (2.5 cases per million doses) may be about 2 to 8.5 times as high as the incidence reported in the 2016 VSD study for all vaccines (1.31 per million doses).”
40. Sellaturay P et al., “Polyethylene glycol (PEG) is a cause of anaphylaxis to the Pfizer/BioNTech mRNA COVID-19 vaccine,” Clin Exp Allergy 2021, 51, 6: 861-863. doi: https://doi.org/10.1111/cea.13874
• “Here, we show polyethylene glycol allergy caused one of the first cases of anaphylaxis to the Pfizer/BioNTech COVID-19 vaccine. Allergy skin prick testing with polyethylene glycol triggered anaphylaxis, highlighting the importance of safety procedures during investigation.”
41. Shi D et al., “To PEGylate or not to PEGylate: Immunological properties of nanomedicine’s most popular component, polyethylene glycol and its alternatives,” Adv. Drug Deliv. Rev. 2022, 180: 114079. doi: https://doi.org/10.1016/j.addr.2021.114079
• “First, phagocytic cells of the immune system are at the forefront of clearance of PEG and PEGylated materials; therefore, toxicity to these cells may influence body’s general defense against infections and damaged or transformed host’s cells. Second, generation of the specific immune response to PEG in the form of antibodies contributes to hypersensitivity reactions (HSRs) to PEG and PEGylated products. Such HSRs include true allergy (IgE mediated, type I hypersensitivity), anaphylactoid reactions (complement-mediated immediate type hypersensitivity or complement-mediated pseudoallergy, CARPA), type II and type III hypersensitivity (IgM and IgG-mediated) reactions. Third, neutralization and cross-reactivity of such antibodies may contribute to HSRs and altered PK of other products containing PEG or other structures similar to PEG.”
42. Somiya M et al., “Sex differences in the incidence of anaphylaxis to LNP-mRNA COVID-19 vaccines,” Vaccine 2021, 39, 25): 3313–3314. doi: 10.1016/j.vaccine.2021.04.066 https://pubmed.ncbi.nlm.nih.gov/34020815/
• “On February 17, 2021, Japan started vaccinating healthcare workers with the Pfizer-BioNTech lipid nanoparticle (LNP)-mRNA COVID-19 vaccine. Among total 79 anaphylaxis cases, 70 cases have been reported in women (89.9%) after 1,096,698 doses of the vaccine until April 4, 2021… Another report confirmed the female predominance of anaphylaxis cases in over 60,000 doses of LNP-mRNA vaccinations; 15 (94%) of the 16 confirmed cases were women… One possible explanation for the sex imbalance is that sensitization to PEG is more common in women due to the relatively frequent exposure to PEG-containing products, such as cutaneous exposure to cosmetics or the use of medications such as contraceptive injections.”
43. Stone CA, Jr., et al., “Immediate Hypersensitivity to Polyethylene Glycols and Polysorbates: More Common Than We Have Recognized,” J Allergy Clin Immunol Pract 2019, 7, 5: 1533-1540.e8. doi: https://doi.org/10.1016/j.jaip.2018.12.003
• “Immediate hypersensitivity to PEG 3350 with cross-reactive polysorbate 80 hypersensitivity may be underrecognized in clinical practice.”
44. Szebeni J et al., “Applying lessons learned from nanomedicines to understand rare hypersensitivity reactions to mRNA-based SARS-CoV-2 vaccines,” Nat. Nanotechnol. 2022, 17: 337–346. doi: https://doi.org/10.1038/s41565-022-01071-x
• “In summary, all the components of LNP–mRNA vaccines… have various immunostimulatory effects… collectively required for vaccine efficacy. The same components, however, also contribute to HSR and other IMAEs…”
45. Tahtinen S and Ira Mellman, “IL-1-mediated inflammation induced by different RNA vaccines is context-specific,” Nature Immunol. 2022, 23, 4: 485-486. doi: https://doi.org/10.1038/s41590-022- 01177-3
• “Systemic inflammatory responses generated by lipid-formulated RNA vaccines are driven by differential induction of pro- and anti-inflammatory interleukin-1 (IL-1) family members in mice and humans… We discovered that the RNA-LPX vaccine induces the release of the cytokine IL-1. IL-1 initiates an innate immune cascade that results in systemic cytokine release and the adverse events that limit vaccine dosing in humans.”
46. Tahtinen S et al., “IL-1 and IL-1ra are key regulators of the inflammatory response to RNA vaccines,” Nat. Immunol. 2022, 23: 532-542. doi: https://doi.org/10.1038/s41590-022-01160-y
• “In human immune cells, RNA vaccines induce production of IL-1 cytokines, predominantly IL-1β, which is dependent on both the RNA and lipid formulation. IL-1 in turn triggers the induction of the broad spectrum of pro-inflammatory cytokines (including IL-6).”
47. Tenchov R et al, “PEGylated Lipid Nanoparticle Formulations: Immunological Safety and Efficiency Perspective,” Bioconjug. Chem. 2023, 34, 6: 941-960. doi: https://doi.org/10.1021/acs.bioconjchem.3c00174
• “A search in the CAS Content Collection identified nearly 900 documents, including ∼150 patents, related to the PEG–lipids immunologically induced adverse effects such as anti-PEG antibodies generation, accelerated blood clearance, and complement activation-related pseudoallergies.”
48. Tinari S, “The EMA covid-19 data leak, and what it tells us about mRNA instability,” BMJ 2021, 372: n672. doi: https://doi.org/10.1136/bmj.n627
• “JW Ulm, a gene therapy specialist who has published on tissue targeting of therapeutic vectors, raised concerns about the biodistribution of LNPs: ‘At present, relatively little has been reported on the tissue localisation of the LNPs used to encase the SARS-CoV-2 spike protein-encoding messenger RNA, and it is vital to have more specific information on precisely where the liposomal nanoparticles are going after injection.’ It is an unknown that Ulm worries could have implications for vaccine safety.”
49. Tran TT and SR Roffler, “Interactions between nanoparticle corona proteins and the immune system,” Curr Opin Biotechnol. 2023, 84: 103010. doi: https://doi.org/10.1016/j.copbio.2023.103010
• “Intravenous administration of pegylated liposomal formulations containing Toll-like receptor agonists to mice on days 0, 4, and 8 resulted in hypersensitivity reaction symptoms…”
50. Troelnikov A et al., “Basophil reactivity to BNT162b2 is mediated by PEGylated lipid nanoparticles in patients with PEG allergy,” J Allergy Clin Immunol. 2021, 148, 1: 91-95. doi: https://doi.org/10.1016/j.jaci.2021.04.032
• “Our findings implicate PEG, as covalently modified and arranged on the vaccine lipid nanoparticle, as a potential trigger of anaphylaxis in response to BNT162b2, and highlight shortcomings of current skin testing protocols for allergy to PEGylated liposomal drugs.”
51. Tsilingiris D et al., “Potential implications of lipid nanoparticles in the pathogenesis of myocarditis associated with the use of mRNA vaccines against SARS-CoV-2,” Metabol. Open 2022, 13: 100159. doi: https://doi.org/10.1016/j.metop.2021.100159
• “The recent observation of a similar adverse event [myocarditis] in a recipient of the non-mRNA, peptide-based NVX-CoV2373 in the frame of a phase III clinical trial with 7020 participants in the active treatment arm raises the question whether the lipid nanoparticle sheath, which is a common structural component of these platforms could be implicated in the pathogenesis of vaccine-induced myocarditis.”
52. Wang H et al., “Polyethylene glycol (PEG)-associated immune responses triggered by clinically relevant lipid nanoparticles in rats,” npj Vaccines 2023, 8: 169. doi: https://doi.org/10.1038/s41541-023-00766-z
• “… ‘antigen-antibody’ complexes may induce severe side effects including hypersensitivity reactions, although the underlying mechanisms have not been fully clarified… Overall, these data provided strong evidence for the dose- and time-dependent induction of anti-PEG IgM.”
53. Wang J et al., “Recent Advances in Lipid Nanoparticles and Their Safety Concerns for mRNA Delivery,” Vaccines 2024, 12, 10: 1148. doi: https://doi.org/10.3390/vaccines12101148
• “… as the immunological activation in response to mRNA-LNP treatment increases, the body’s defense capability may also rise, but there is a high possibility of the mRNA-LNP complexes causing adverse effects, including allergies and autoimmune diseases.”
54. Warren CM et al.” Assessment of Allergic and Anaphylactic Reactions to mRNA COVID-19 Vaccines With Confirmatory Testing in a US Regional Health System,” JAMA Netw. Open. 2021, 4, 9: e2125524. doi: 10.1001/jamanetworkopen.2021.25524 https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2784268
• “These findings suggest that non–IgE-mediated allergic reactions to PEG may be responsible for many documented cases of allergy to mRNA vaccines.”
55. Yang M et al., “Effects of PEG antibodies on in vivo performance of LNP-mRNA vaccines,” Int J Pharm. 2024, 650: 123695. doi: https://doi.org/10.1016/j.ijpharm.2023.123695
• “PEG antibodies binding on the LNP vaccine increased probability of complement activation in animal as well as in human serum and led to lethal side effect in large dosage via intravenous injection of mice. Our data suggested that PEG antibodies in human was a risky factor of LNP-based vaccines for biosafety concerns but not efficacy.”
56. Yuan Z et al., “Impact of physicochemical properties on biological effects of lipid nanoparticles: Are they completely safe,” Sci Total Environ. 2024, 927: 172240. doi: https://doi.org/10.1016/j.scitotenv.2024.172240
• “The physicochemical properties of LNPs, like size, surface hydrophobicity, surface charge, surface modification and lipid composition, determine the interaction of LNPs with macromolecules and organelles to a large extent, resulting in negative effects on cells, especially cytotoxicity and genotoxicity, and cell death.”
57. Zhou ZH et al ., “Anti-PEG IgE in anaphylaxis associated with polyethylene glycol,” J Allergy Clin Immunol Pract 2021, 9, 4: 1731-1733.e3. doi: 10.1016/j.jaip.2020.11.011 https://pubmed.ncbi.nlm.nih.gov/33217616/
• “… all the anaphylaxis case samples and none of the control samples were clearly positive for anti-PEG IgE.”
Appendix B
World Council for Health joins 10 Nordic and Baltic Countries (“The NORTH Group”) in calling for immediate suspension of the COVID-19 mRNA Vaccines
Notice of extreme concern regarding the safety of COVID-19 modified mRNA vaccines.
On November 25th, 2024 an international group of politicians and leading medical and other professionals wrote to the heads of state of 10 European countries (Denmark, Estonia, Finland, Greenland, Iceland, Latvia, Lithuania, Norway, Sweden, and the United Kingdom) calling for a suspension of all modified mRNA vaccines citing serious health concerns.
The call builds upon a similar initiative in Australia brought by Mr. Russell Broadbent MP, and is supported by a scientific lay summary citing that:
COVID-19 modified mRNA vaccines have resulted in unprecedented levels of side effects including death. Reproducible analyses of public data shows that it was a lottery as to which batch a person received and the side effects they experienced.
Vaccines were never tested for their ability to block transmission. Hence, medical product regulators, as well as government agencies, misled the public when coercing the acceptance of these products.
Multiple independent analyses now show that modified mRNA vaccines contain variable and unprecedented levels of residual DNA, raising extreme concerns for risks to human health and the potential for genetic damage.
The call has very strong international support and demands:
An immediate halt to the use of modified mRNA vaccines.
An independent and transparent investigation into their approval and use.
Scientific evidence that shows that there is no risk of damage to human DNA.
Heads of state and public health leaders are asked to respond to the following questions:
What is required to set up an independent and transparent forensic enquiry into the regulatory processes leading to the approval of modified mRNA vaccines?
Is there anything that prevents the initiation and prioritization of research into potential links between modified mRNA vaccines and cancer, infertility, or other chronic diseases?
Governments and regulatory bodies throughout the world need to respond appropriately to protect the well-being of their citizens.
Full press release including the named signatories:
https://northgroup.info/pdfs/NORTH_Group_Letter-2024-11-25.pdf
Scientific Lay Summary
https://northgroup.info/pdfs/NORTH_Group_Summary-2024-11-25_UK.pdf
Appendix C – The Hope Accord
the hope accord
https://thehopeaccord.org/
WE, THE UNDERSIGNED HEALTHCARE PROFESSIONALS, SCIENTISTS
AND CONCERNED MEMBERS OF THE PUBLIC, CALL FOR:
1. THE IMMEDIATE SUSPENSION OF THE COVID-19 mRNA VACCINE PRODUCTS
A growing body of evidence suggests that the widespread rollout of the novel Covid-19 mRNA vaccine products is contributing to an alarming rise in disability and excess deaths.
The association observed between the vaccine rollout and these concerning trends is now supported by additional significant findings. These include the discovery of plausible biological mechanisms of harm demonstrated in laboratory and autopsy studies, as well as high rates of adverse events seen in randomized clinical trials and national surveillance programs. Altogether, these observations indicate a causal link.
This new technology was granted emergency use authorization to address a situation that no longer exists. Going forward, the burden of proof falls on those still advocating for these products to compellingly demonstrate that they aren’t resulting in net harm. Until such evidence is presented, regulators should suspend their use as a matter of standard medical precaution.
2. A COMPREHENSIVE RE-EVALUATION OF THE SAFETY AND EFFICACY OF ALL COVID-19 VACCINE PRODUCTS
Independent investigations must be properly resourced to allow a comprehensive re-evaluation of all Covid-19 vaccine products.
There must be a full exploration of mechanisms of harm to provide insight into their impact on the human body, both short and long term. Effectiveness must be reassessed through a comprehensive review of actual clinical impact on illness and mortality, as opposed to synthetic results based on modelled assumptions.
We call on the scientific community to come forward with findings from unpublished Covid-19 vaccine studies. This will help mitigate publication bias, whereby unfavorable results were often rejected or withheld due to fears of reputational damage. Crucially, government bodies and the pharmaceutical industry must also provide full transparency, granting access to previously undisclosed anonymized patient-level data from clinical trials and surveillance programs.
These cumulative actions will help determine any real world benefit of these products versus the true extent of the damage caused.
3. THE IMMEDIATE RECOGNITION AND SUPPORT FOR THE VACCINE-INJURED
The denial of vaccine injury is a betrayal of those who followed official directives, often under coercion from mandates restricting their access to work, education, travel, hospitality and sports.
The vaccine-injured must be recognized and every effort made to understand their conditions. Support should include readily accessible multidisciplinary clinics offering investigation and treatment as well as appropriate compensation for all those who have been harmed.
4. THE RESTORATION OF ETHICAL PRINCIPLES ABANDONED DURING THE COVID-19 ERA
Fundamental and cherished principles of medical ethics were disregarded on the premise of an emergency. These included: ‘first do no harm’, informed consent, bodily autonomy and the notion that adults protect children – not the other way around. The precautionary principle was inverted. Also, particularly concerning was the erosion of free speech – a democratic principle that underpinned the ability to question untested interventions whilst ensuring other principles were upheld. The consequence was exposing the public, especially healthy young people – including children – to unacceptable risks of harm.
Emergencies are never a reason to abandon our principles; it is precisely at such times that we most profoundly depend on them. Only after acknowledging they were wrongly abandoned can we commit to upholding them consistently and in doing so, better protect future generations.
5. ADDRESSING THE ROOT CAUSES OF OUR CURRENT PREDICAMENT
The medical profession must lead by admitting we lost our way.
By drawing attention to these medical and ethical issues surrounding the Covid-19 response, we hope to validate and amplify the call to establish the relevant facts and ensure vital lessons are learned.
An honest and thorough investigation is needed, addressing the root causes that have led us to this place, including institutional groupthink, conflicts of interest and the suppression of scientific debate.
We ultimately seek a renewed commitment to the core principles of ethical medicine, returning to an era in which we strive for transparency, accountability and responsible decision-making throughout the spheres of medicine and public health.
ON 3 JULY 2024, THIS ACCORD WAS AGREED AND SIGNED BY:
(alphabetically)
67,105
TOTAL SUPPORTERS
1986 MEDICAL DOCTORS
5908 OTHER HEALTHCARE PROFESSIONALS
2103 SCIENTISTS & ACADEMICS
57108 CONCERNED CITIZENS
Dr Clare Craig
Diagnostic Pathologist
Dr Suneel Dhand
Internal Medical Physican
Dr Joseph Fraiman
Emergency Physican
Dr Charles Hoffe
Family Physician
Dr Timothy Kelly
Medical Doctor & Systems Analyst
Dr Jeyanthi Kunadhasan
Anaesthetist
Dr Aseem Malhotra
Cardiologist
Dr Ayiesha Malik
General Practitioner
Dr. Dean Patterson
Cardiologist
Mr. T James Royle
General and Colorectal Surgeon
Dr Jackie Stone
Medical Education Director
Prof Bret Weinstein
Evolutionary Biologist
The Hope Accord provides the following information for further context and understanding.
Growing Body of Evidence
The Hope Accord refers to a “growing body of evidence” suggesting concerns about modified mRNA products. While the full extent of this evidence encompasses hundreds of studies and reports, we provide here a selection of resources that together offer comprehensive overviews and analyses of the available data.
People’s Vaccine Enquiry Witness Statements (https://peoplesvaccineinquiry.co.uk/statements/ ) A UK initiative providing expert testimony on COVID-19 vaccines. Several Hope Accord founders contributed, including:
“Unsafe and Defective” by Clare Craig (2024) Comprehensive aggregation of key evidence related to concerns raised in the Hope Accord. (https://peoplesvaccineinquiry.co.uk/wp-content/uploads/2024/06/HART-Witness-Statement-Dr-Clare-Craig.pdf )
Doctors for Patients UK (DfPUK) Testimonies (2024) Observations from some of the UK Hope Accord founders, based on professional experiences and data analyses. (https://peoplesvaccineinquiry.co.uk/wp-content/uploads/2024/06/DFP-FINAL-short-statement-3.pdf) [see Table of Contents and excerpts below]
“Curing the Pandemic of Misinformation on COVID-19 mRNA Vaccines Through Real Evidence-Based Medicine – Part 1” by Aseem Malhotra (2022) Reviews evidence from trials and real-world data on mRNA COVID vaccines, highlighting risk-benefit concerns and informed consent issues.(https://journalofmetabolichealth.org/index.php/jmh/article/view/71)
“Serious Adverse Events of Special Interest Following mRNA Vaccination in Randomized Trials” by Joseph Fraiman et al. (2022) Reanalyses Pfizer and Moderna trial data, finding an excess risk of serious adverse events in mRNA vaccine recipients compared to placebo groups. (https://www.sciencedirect.com/science/article/pii/S0264410X22010283)
Root-Cause Analysis
The following resources delve into the underlying systemic and cultural factors that contributed to the issues addressed by the Hope Accord:
“Curing the Pandemic of Misinformation on COVID-19 mRNA Vaccines Through Real Evidence-Based Medicine – Part 2” by Aseem Malhotra (2022)Examines root causes of public health failures during the pandemic, discussing regulatory capture and the need to rebuild trust in health institutions. (https://journalofmetabolichealth.org/index.php/jmh/article/view/72/228)
Beyond Blame: Dissecting the Systemic Roots of Societal Disease of the Covid Era by Tim Kelly (2024)Explores factors leading to current issues, including hyper-specialisation and centralisation. Proposes priorities for addressing the crisis. (https://www.thehopeaccord.org/BeyondBlame)
Appendix D
Doctors for Patients UK (DfPUK) Testimonies (2024)
Established in September 2022, Doctors for Patients UK (DfPUK) was formed by a group of doctors alarmed by the disregard of medical ethics—a trend that endangers patient care and eroded public trust amid the Covid-19 pandemic.
A primary concern among DfPUK members is the safety and ethical implications of Covid-19 vaccines, particularly regarding vulnerable populations such as children and pregnant women.
[…]
DfPUK has prepared this submission for "The People’s Vaccine Inquiry" as part of a moral and public duty to address these issues, in alignment with GMC mandates that require doctors to act when patient safety is at risk.
After reviewing member testimonies, the authors reaffirmed their conclusion that the risks of mRNA and other Covid-19 vaccines outweigh their benefits. This further analysis compelled the creation of The Hope Accord, a petition that calls for an immediate halt and re-evaluation of these products.
The petitioner urges the FDA to review the complete DfPUK Testimonies report as it contains numerous important clinical observations relevant to this petition.
https://peoplesvaccineinquiry.co.uk/wp-content/uploads/2024/06/DFP-FINAL-short-statement-3.pdf
Appendix E
The Association of American Physicians and Surgeon (AAPS) Statement Calling for Moratorium on COVID-19 Shot Mandates and Genetic Injections
https://aapsonline.org/aaps-statement-calling-for-moratorium-on-covid-19-injections-and-mandates/
Originally Published March 21, 2023
1. COVID 19 injections are under Emergency Use Authorization and must be considered experimental. Informed consent is a bedrock principle of medical ethics, yet millions of people have taken COVID-19 injections under duress.
2. The long-term effects of the novel mRNA or DNA technology and the lipid nanoparticles involved in their administration – including carcinogenesis, mutagenesis, autoimmune phenomena, and impairment of fertility – cannot possibly be known.
3. There are numerous safety signals, including excess sudden deaths, that would in the past have prompted immediate withdrawal of vaccines or drugs from the market.
4. The expected intensive, sophisticated investigations of reported adverse effects associated with COVID-19 vaccination, including myocarditis, pericarditis, paralysis, thromboembolism, menstrual abnormalities, and unusual cancers, have not been undertaken.
5. COVID-19 genetic injections have not been shown in randomized, controlled trials to be effective in preventing infection, transmission, hospitalization or death.
6. In children who have virtually zero likelihood of death from COVID, there is no evidence of benefit exceeding risks for these products.
7. Regulatory agencies are corrupted by conflicts of interest, lack of transparency, and lack of accountability.
8. Vaccine-injured patients have little if any expectation of compensation, and manufacturers are shielded from liability. This liability protection must be ended.
9. All mandates, including requirements for school attendance or work, should immediately be withdrawn.
10. COVID-19 genetic injections should be withdrawn from the market.
Appendix F – Doctors for COVID Ethics
1. The Dangers of RNA-Vaccines
by Sucharit Bhakdi MD, Karina Reiss PhD and Michael Palmer MD
This open letter explains the dangers posed by mRNA vaccines, namely, that cells and tissues which take up the vaccine particles will suffer destruction at the hands of the immune system, and furthermore that cells which evade destruction may end up being genetically modified. The risk of genetic modification also pertains to egg and sperm cells and therefore to future generations. Both risks are inherent in this vaccine technology — they are not limited to the mRNA vaccines against COVID-19 alone.
The novel concept of RNA-vaccines
Chromosomes are the books of life containing DNA-encoded recipes for the production of protein molecules. When needed, the book is opened and a copy of the required recipe is made. The copy is mRNA, which directs production of the protein, after which it is disposed of.
RNA vaccines are such short-lived copies of chromosomal recipes that direct the production of selected antigens, e.g. the SARS-CoV-2 spike protein. More than one billion copies (RNA molecules) are administered with each injection. Mass production of mRNA requires mass availability of the DNA recipes. How can this be achieved?
The solution represents a founding pillar of gene technology. The billions and trillions of copies of the DNA recipes are derived from bacteria. The recipes are contained in minute, bacterial chromosomes that are termed plasmids. The division time of the bacteria is approximately 20 minutes – the number of cells increase approximately eightfold every hour. Literally countless bacteria with the plasmids can therefore be harvested from fluid culture in just a few days.
Plasmids are easily manipulated. Foreign recipes, i.e. genes such as those encoding for viral proteins can be inserted. Following bacterial multiplication, the plasmids are harvested and used as the templates for production of the mRNA copies.
The RNA molecules are then packaged into tiny fatty globules termed lipid nanoparticles (LNP). The essential components of LNP are man-made and potentially highly toxic. Their use in humans was forbidden prior to 2020. This rule was violated with the emergency use approval of the COVID RNA-vaccines. The packaging material is essential to protect RNA from destruction so that it can travel in the bloodstream to reach all organs of the body. There the globules act as Trojan horses. They are taken up by cells and their cargo is then released. Production of the spike protein and triggering of the immune response follow, leading to formation of specific antibodies that are supposed to protect against future infections.
The fatal flaw
The immune system recognizes and destroys body cells that produce foreign proteins, such as occurs when they become infected with viruses. This ability to recognize non-self is given at birth. It protects us throughout life because virus-infected cells are thus effectively eliminated. It cannot be suppressed. Therefore, if mRNA coding for any non-self protein is introduced into a cell, that cell will come under attack by the immune system. This is the fatal flaw that underlies the whole concept. The numbers of packaged RNA copies administered with each injection are gigantic. Myriad immune attack events will erupt throughout the body that can only halt when production of the alien protein comes to an end. How long will this take? A few days, as the vaccine manufacturers and regulatory authorities repeatedly asserted?
The ultimate catastrophe
An alarming finding surfaced over the past year that was irreconcilable with that assertion. Spike protein and multiorgan inflammation was detected in vaccinees weeks and even months after the injections (1-3). And this was associated with severe and often fatal illness (2,3). What earthly reason could there have been and could there still be for long-lasting production of an RNA-encoded protein and inflammation?
A possible and extremely terrifying answer came with the recent discovery of McKernan and colleagues (4). In the vaccine production process, the plasmid-DNA templates must be removed from the generated mRNA before the latter is packaged into LNPs.. Otherwise, plasmids will also end up in the fat globules. McKernan discovered that this crucial step of removing plasmid-DNA had not been assiduously undertaken. Huge amounts of plasmid-DNA were found in packaged form that guaranteed their successful delivery to cells, where they would be able to function for extended time periods.
Cellular uptake of a functional foreign chromosome equates with nothing less than genetic alteration. This must be the fate of humans who are injected with packaged bacterial plasmids. In addition, expression of the alien gene will invoke immune attack on the producing cells. Continued and prolonged production of the non-self protein will intensify the organ damage and inflammation. This will happen throughout the body. Blood clots will form as vessels get injured and tissues will die for lack of oxygen. The heart is one organ that cannot replace dead cells. Who has not heard of the mysterious sudden cardiac deaths that are occurring around the world? They are only the tip of an iceberg. Vaccine-induced heart disease has entered the daily agenda of young and old. The second organ that cannot replace its dead cells is the brain. Depending on where vaccine damage is done, any neurological and psychiatric affliction may follow.
Analogous autoimmune-like diseases can develop simultaneously in different organs. This multifaceted feature of vaccination-induced injury is unique and tellingly illustrated in the tragic case of a 14-year old child who died of multi-organ inflammation as has never been seen before (5).
The potential of vaccination to negatively impact on fertility and reproduction is enormous. The vaccines accumulate in the reproductive organs and this could immediately impair fertility. Uptake of circulating RNA and DNA by cells of the placenta could result in stillbirths. Placental damage may also enable the packaged genes to enter the fetal circulation. Stem cells in umbilical cord blood are reduced and impaired following vaccination (6), and it must be feared that this is because the baby is reached in the mother’s womb. The fat globules with their cargo are also known to find their way into breast milk (7). Gut permeability is high during the first weeks after birth (8), and the terrible possibility exists that breast-feeding will result in direct passage of vaccines into the baby, where suicide mechanisms may be triggered.
In the laboratory, it is possible to insert plasmid DNA into the book of life. If this occurs in vaccinated humans, the possible consequences are unending. Disruption of the exquisitely tuned network that controls cell division and differentiation can lead to cancer. Mutations in sperm and fertilized egg cells could render altered traits inheritable and lead to the creation of beings that have departed from the evolutionary track of the human race.
Conclusion
Widespread and sustained injury to tissues and to blood vessels must be expected to occur through attack of the immune system on spike protein-producing cells. This attack occurs because the spike protein is non-self; and since every other mRNA vaccine will encode non-self, we must expect that it will cause harm by the same mechanism and to a similar extent. These nightmarish scenarios will worsen with every booster injection.
To top everything, contamination of vaccine batches with functional plasmid-DNA must be expected to be the rule and not the exception, because no cost-effective procedure exists to reliably separate mass-produced RNA from the plasmids. The introduction of a foreign chromosome equates with alteration of the genome. Long-lasting auto-immune attack on the cells is inevitable.
Integration of plasmid-DNA into the human chromosome must moreover be expected to occasionally occur. Myriad cellular functions can then be permanently disrupted. Malignancies may arise and life expectancy may drop. A horror scenario arises that could affect countless people whom we love and hold in our hearts. We must prevent this.
The medical world must rise on the spot and bring the use of RNA-injections to a full stop.
References
1. Bansal S. et al. (2021) Cutting Edge: Circulating Exosomes with COVID Spike Protein Are Induced by BNT162b2 (Pfizer-BioNTech) Vaccination prior to Development of Antibodies: A Novel Mechanism for Immune Activation by mRNA Vaccines. J Immunol 207:2405-2410.
2. Mörz M. (2022) A Case Report: Multifocal Necrotizing Encephalitis and Myocarditis after BNT162b2 mRNA Vaccination against COVID-19. Vaccines 10:1651.
3. Bhakdi, S. and Burkhardt, A. (2021) On COVID vaccines: why they cannot work, and irrefutable evidence of their causative role in deaths after vaccination. https://doctors4covidethics.org/on-covid-vaccines-why-they-cannot-work-and-irrefutable-evidence-of-their-causative-role-in-deaths-after-vaccination/
4. McKernan K. (2023) Sequencing of bivalent Moderna and Pfizer mRNA vaccines reveals nanogram to microgram quantities of expression vector dsDNA per dose. https://osf.io/b9t7m/
5. Nushida H. et al. (2023) A case of fatal multi-organ inflammation following COVID-19 vaccination. Leg Med 63: 102244.
6. Estep B.K. et al. (2023) Skewed fate and hematopoiesis of CD34+ HSPCs in umbilical cord blood amid the COVID-19 pandemic. iScience 25: 105544.
7. Hanna N. et al. (2022) Detection of Messenger RNA COVID-19 Vaccines in Human Breast Milk. JAMA Pediatr. 176:1268-1270.
8. Weström B. et al. (2020) The Immature Gut Barrier and Its Importance in Establishing Immunity in Newborn Mammals. Front Immunol. 11:1153.
In addition, below we provide a curated selection of relevant publications and other written materials by Doctors for Covid Ethics and signatories believed to be relevant by the petitioner.
Alternate mechanisms of mRNA vaccine toxicity: which one is the main culprit? This paper summarizes the mode of action of mRNA vaccines, as well as three potential pathogenetic mechanisms: chemical toxicity of lipid nanoparticles, direct toxicity of the spike protein, and the destructive effects of the immune response to the spike protein. The third mechanism is likely the most important one. If this conclusion is correct, then essentially the same level of toxicity must be expected with future mRNA vaccines against any other pathogenic microbes. (https://doctors4covidethics.org/alternate-mechanisms-of-mrna-vaccine-toxicity-which-one-is-the-main-culprit/)
COVID-19 mRNA vaccines contain excessive quantities of bacterial DNA: evidence and implications Recent studies by Kevin McKernan, a leading expert in sequencing methods for DNA and RNA, have revealed that batches of the modified mRNA vaccines produced by both Pfizer and Moderna contain a high proportion of contaminating bacterial DNA. This document summarizes the evidence of that DNA contamination and discusses what possible health risks it implies to the recipients of the vaccines. (https://doctors4covidethics.org/covid-19-mrna-vaccines-contain-excessive-quantities-of-bacterial-dna-evidence-and-implications/)
Immunology 101: why intramuscular COVID-19 vaccination must fail This paper explains the fundamental reason why such cases had to be expected: the antibodies induced by intramuscular vaccination will only circulate in the bloodstream, but they will not reach the surface of the mucous membranes in the upper airways. We also briefly discuss possible mechanisms of vaccine-induced immunopathology. (https://doctors4covidethics.org/immunology-101-why-intramuscular-covid-19-vaccination-must-fail/)
Elementary, my dear Watson: why mRNA vaccines are a very bad idea This short article explains from first principles why adverse events must be expected not just after the first injection of such a vaccine but after each booster shot as well. The argument is not limited to SARS-CoV-2 or its spike protein but applies generally to any non-self antigen introduced in the form of mRNA. (https://doctors4covidethics.org/elementary-my-dear-watson-why-mrna-vaccines-are-a-very-bad-idea/)
mRNA vaccines against COVID-19 and their effects on the central nervous system This document answers three questions: 1. What evidence is currently available to show that mRNA vaccine particles cross the blood-brain barrier? 2. How long can the vaccine nanoparticles remain in the brain? 3. What damage can vaccine nanoparticles cause to the brain? (https://doctors4covidethics.org/mrna-vaccines-against-covid-19-und-their-effects-on-the-central-nervous-system/)
Vascular and organ damage induced by mRNA vaccines: irrefutable proof of causality This article summarizes evidence from experimental studies and from autopsies of patients deceased after vaccination. (https://doctors4covidethics.org/vascular-and-organ-damage-induced-by-mrna-vaccines-irrefutable-proof-of-causality/)
Did Pfizer Perform Adequate Safety Testing for its Covid-19 mRNA Vaccine in Preclinical Studies? Evidence of Scientific and Regulatory Fraud by Sasha Latypova This extensive review illustrates the complete breakdown of the regular process of drug development and approval, previously known to be rigorous and ethical, as well as the shocking negligence on the part of the regulatory agencies which are supposed to keep the pharmaceutical manufacturers honest. (https://doctors4covidethics.org/did-pfizer-perform-adequate-safety-testing-for-its-covid-19-mrna-vaccine-in-preclinical-studies-evidence-of-scientific-and-regulatory-fraud/)
Investigation of metallic contaminations found in vector- and mRNA-based COVID-19-”vaccines”: Preliminary Results Three of the four gene-based COVID-19 “vaccines” are contaminated with an abundance of metallic particles. The contaminations alone are reason enough to halt the manufacture of these “vaccines.” (https://doctors4covidethics.org/investigation-of-metallic-contaminations-found-in-vector-and-mrna-based-covid-19-vaccines-preliminary-results/)
The Pfizer mRNA Vaccine: Pharmacokinetics and Toxicity In this detailed analysis, Associate Professor Michael Palmer and Professor Sucharit Bhakdi explain the existing evidence and science behind the toxicity and pharmacokinetics of mRNA vaccines. (https://doctors4covidethics.org/the-pfizer-mrna-vaccine-pharmacokinetics-and-toxicity/)
750+ Studies About the Dangers of the COVID-19 Injections Kyle Beattie has shared this extensive curated list of literature references on COVID-19 “vaccine” adverse effects from 2021 and early 2022. (https://doctors4covidethics.org/750-studies-about-the-dangers-of-the-covid-19-injections/
Appendix G - Florida Surgeon General Calls for Halt in Use of COVID-19 mRNA Vaccines
January 03, 2024 Statement
https://www.floridahealth.gov/newsroom/2024/01/20240103-halt-use-covid19-mrna-vaccines.pr.html
Tallahassee, FL — On December 6, 2023, Florida State Surgeon General Dr. Joseph A. Ladapo sent a letter to the United States Food and Drug Administration (FDA) Commissioner Dr. Robert M. Califf and Center for Disease Control and Prevention (CDC) Director Dr. Mandy Cohen regarding questions pertaining to the safety assessments and the discovery of billions of DNA fragments per dose of the Pfizer and Moderna COVID-19 mRNA vaccines.
The Surgeon General outlined concerns regarding nucleic acid contaminants in the approved Pfizer and Moderna COVID-19 mRNA vaccines, particularly in the presence of lipid nanoparticle complexes, and Simian Virus 40 (SV40) promoter/enhancer DNA. Lipid nanoparticles are an efficient vehicle for delivery of the mRNA in the COVID-19 vaccines into human cells and may therefore be an equally efficient vehicle for delivering contaminant DNA into human cells. The presence of SV40 promoter/enhancer DNA may also pose a unique and heightened risk of DNA integration into human cells.
In 2007, the FDA published guidance on regulatory limits for DNA vaccines in the Guidance for Industry: Considerations for Plasmid DNA Vaccines for Infectious Disease Indications (Guidance for Industry). In this Guidance for Industry, the FDA outlines important considerations for vaccines that use novel methods of delivery regarding DNA integration, specifically:
DNA integration could theoretically impact a human’s oncogenes – the genes which can transform a healthy cell into a cancerous cell.
DNA integration may result in chromosomal instability.
The Guidance for Industry discusses biodistribution of DNA vaccines and how such integration could affect unintended parts of the body including blood, heart, brain, liver, kidney, bone marrow, ovaries/testes, lung, draining lymph nodes, spleen, the site of administration and subcutis at injection site.
On December 14, 2023, the FDA provided a written response providing no evidence that DNA integration assessments have been conducted to address risks outlined by the FDA themselves in 2007. Based on the FDA’s recognition of unique risks posed by DNA integration, the efficacy of the COVID-19 mRNA vaccine’s lipid nanoparticle delivery system, and the presence of DNA fragments in these vaccines, it is essential to human health to assess the risks of contaminant DNA integration into human DNA. The FDA has provided no evidence that these risks have been assessed to ensure safety. As such, Florida State Surgeon General Dr. Joseph A. Ladapo has released the following statement:
“The FDA’s response does not provide data or evidence that the DNA integration assessments they recommended themselves have been performed. Instead, they pointed to genotoxicity studies – which are inadequate assessments for DNA integration risk. In addition, they obfuscated the difference between the SV40 promoter/enhancer and SV40 proteins, two elements that are distinct.
DNA integration poses a unique and elevated risk to human health and to the integrity of the human genome, including the risk that DNA integrated into sperm or egg gametes could be passed onto offspring of mRNA COVID-19 vaccine recipients. If the risks of DNA integration have not been assessed for mRNA COVID-19 vaccines, these vaccines are not appropriate for use in human beings. […]
September 12, 2024 Statement
On September 12, 2024, following up on the guidance cited above, the Florida State Surgeon General reiterated the recommendation against the use of mRNA COVID-19 vaccines and outlined a number of specific safety and efficacy concerns:
Updated Guidance for COVID-19 Boosters for the Fall and Winter 2024–2025 Season
Tallahassee, Fla. – The Florida Department of Health (Department) is reminding health care providers of the importance of remaining up to date with current literature related to COVID-19 vaccines and boosters, and the importance of providing patients with informed consent.
On August 22, 2024, the United States Food and Drug Administration (FDA) approved and authorized updated versions of mRNA vaccines from Pfizer-BioNtech and Moderna. The FDA approved the vaccine for people 12 and older and provided emergency use authorization for children 6 months to 11 years old. The stated target of these boosters is the Omicron variant which is not causing a significant number of infections.
The most recent booster approval was granted in the absence of booster-specific clinical trial data performed in humans. Furthermore, this booster does not protect against the currently dominant strain, accounting for approximately 37% of infections in the United States. There are currently limited data to inform whether these boosters offer any substantial protection against the virus and subsequent circulating variants. Although randomized clinical trials are normally used to approve therapeutics, the federal government has not required COVID-19 vaccine manufacturers to demonstrate their their boosters prevent hospitalizations or death from COVID-19 illness.
Additionally, the federal government has failed to provide sufficient data to support the safety and efficacy of COVID-19 boosters, or acknowledge previously demonstrated safety concerns associated with COVID-19 vaccines and boosters, including:
prolonged circulation of mRNA and spike protein in some vaccine recipients,
increased risk of lower respiratory tract infections, and
increased risk of autoimmune disease after vaccination.
[…] Based on the high rate of global immunity and currently available data, the State Surgeon General advises against the use of mRNA COVID-19 vaccines. Any provider concerned about the health risks associated with COVID-19 for patients over the age of 65 or with underlying health conditions should prioritize patient access to non-mRNA COVID-19 vaccines and treatment.
Safety and Efficacy Concerns
Providers and patients should be aware of outstanding mRNA COVID-19 vaccine safety and efficacy concerns:
The mRNA COVID-19 vaccines present a risk of subclinical and clinical myocarditis and other cardiovascular conditions among otherwise healthy individuals.
The mRNA COVID-19 vaccine may be associated with an increased risk of postural orthostatic tachycardia syndrome (POTS).
The mRNA COVID-19 vaccine may be associated with an increased risk of autoimmune diseases including systemic lupus erythematosus (SLE), rheumatoid arthritis, and psoriasis.
Throughout the pandemic, studies across geographic regions found that the mRNA COVID-19 vaccines are associated with negative effectiveness after four to six months. As efficacy waned, studies showed that COVID-19 vaccinated individuals developed an increased risk for infection.
Elevated levels of mRNA and spike protein from the mRNA COVID-19 vaccine persist among some individuals for an indefinite period, which may carry health risks.
Potential DNA integration from the mRNA COVID-19 vaccines pose unique and elevated risk to human health and to the integrity of the human genome, including the risk that DNA integrated into sperm or egg gametes could be passed onto offspring of mRNA COVID-19 vaccine recipients.
There is unknown risk of potential adverse impacts with each additional dose of the mRNA COVID-19 vaccine; currently individuals may have received five to seven doses (and counting) of this vaccine over a 3-year period.
Appendix H
Attorney General Ken Paxton Sues Pfizer for Misrepresenting COVID-19 Vaccine Efficacy and Conspiring to Censor Public Discourse
Texas Attorney General Ken Paxton has sued Pfizer, Inc., for unlawfully misrepresenting the effectiveness of the company’s COVID-19 vaccine and attempting to censor public discussion of the product.
Pfizer engaged in false, deceptive, and misleading acts and practices by making unsupported claims regarding the company’s COVID-19 vaccine in violation of the Texas Deceptive Trade Practices Act.
The pharmaceutical company's widespread representation that its vaccine possessed 95% efficacy against infection was highly misleading. That metric represented a calculation of the so-called “relative risk reduction” for vaccinated individuals in Pfizer’s initial, two-month clinical trial results. FDA publications indicate “relative risk reduction” is a misleading statistic that “unduly influence[s]” consumer choice. Pfizer was also put on notice at that time that vaccine protection could not accurately be predicted beyond two months. Nevertheless, Pfizer fostered a misleading impression that vaccine protection was durable and withheld from the public information that undermined its claims about the duration of protection. And, despite the fact that its clinical trial failed to measure whether the vaccine protects against transmission, Pfizer embarked on a campaign to intimidate the public into getting the vaccine as a necessary measure to protect their loved ones.
In fact, Pfizer’s product failed to live up to the company’s representations. COVID-19 cases increased after widespread vaccine administration, and some areas saw a greater percentage of deaths from COVID-19 among the vaccinated population than the unvaccinated. When the failure of its product became apparent, Pfizer then pivoted to silencing truth-tellers. The lawsuit notes: “How did Pfizer respond when it became apparent that its vaccine was failing and the viability of its cash cow was threatened? By intimidating those spreading the truth, and by conspiring to censor its critics. Pfizer labeled as ‘criminals’ those who spread facts about the vaccine. It accused them of spreading ‘misinformation.’ And it coerced social media platforms to silence prominent truth-tellers.”
“We are pursuing justice for the people of Texas, many of whom were coerced by tyrannical vaccine mandates to take a defective product sold by lies,” said Attorney General Paxton. “The facts are clear. Pfizer did not tell the truth about their COVID-19 vaccines. Whereas the Biden Administration weaponized the pandemic to force illegal public health decrees on the public and enrich pharmaceutical companies, I will use every tool I have to protect our citizens who were misled and harmed by Pfizer’s actions.”
The lawsuit follows Attorney General Paxton’s investigation into Pfizer and other vaccine manufacturers announced earlier this year.
Please review the lawsuit in full at: www.texasattorneygeneral.gov/sites/default/files/images/press/Pfizer%20Vaccine%20Petition%20Filed.pdf
Appendix I
The Scientific Publications Directory located at www.react19.org/science is a vast collection of peer reviewed case reports and studies citing adverse effects post COVID vaccination.
The curators write, “Researching Covid vaccine adverse events can be daunting in part due to a broad myriad of factors. Primarily, the information is incredibly challenging to find. Here, we share an ever growing list of peer-reviewed studies specific to Covid vaccine adverse events. This list is curated and maintained by our dedicated staff of injured PhDs and medical professionals.”
While our petition lacks the capacity to integrate this massive database of reports and studies, the petitioner strongly urges the FDA to systematically review and consider the entirety of the contents of the React19.org/Science database as part of the comprehensive safety review.
ENDNOTES
[1] Shibata H, Nomura Y, Kawakami T, Yamamoto E, Ando D, Uchiyama N, Tokumoto H, Koide T, Sakoda H, Yoshida H, Abe Y, Hakamatsuka T, Ikarashi Y, Haishima Y, Ishii-Watabe A, Izutsu KI, Honma M, Goda Y. [Investigation of Foreign Particles in Moderna COVID-19 Vaccine]. Yakugaku Zasshi. 2022;142(8):867-874. Japanese. doi: 10.1248/yakushi.22-00067. PMID: 35908947.
[2] Wingrove P. Exclusive: US FDA finds control lapses at Moderna manufacturing plant. Reuters. December 15, 2023. https://www.reuters.com/business/healthcare-pharmaceuticals/us-fda-finds-control-lapses-moderna-manufacturing-plant-2023-12-15
[3] Florida Department of Health. Florida State Surgeon General Calls for Halt in the Use of COVID-19 mRNA Vaccines. Jan. 03, 2024. https://www.floridahealth.gov/newsroom/2024/01/20240103-halt-use-covid19-mrna-vaccines.pr.html
[4] Florida Department of Health. Updated Guidance for COVID-19 Boosters for the Fall and Winter 2024–2025 Season. Sept. 12, 2024. https://www.floridahealth.gov/newsroom/2024/09/20210912-UpdatedGuidanceCOVID-19.html
[5] Buergin N, Lopez-Ayala P, et al. Sex-specific differences in myocardial injury incidence after COVID-19 mRNA-1273 booster vaccination. European Journal of Heart Failure. July 20, 2023. https://onlinelibrary.wiley.com/doi/10.1002/ejhf.2978
[6] Mansanguan S, Charunwatthana P, Piyaphanee W, Dechkhajorn W, Poolcharoen A, Mansanguan C. Cardiovascular Manifestation of the BNT162b2 mRNA COVID-19 Vaccine in Adolescents. Tropical Medicine and Infectious Disease. 2022; 7(8):196. https://doi.org/10.3390/tropicalmed7080196
[7] Kwan, A.C., Ebinger, J.E., Wei, J. et al. Apparent risks of postural orthostatic tachycardia syndrome diagnoses after COVID-19 vaccination and SARS-Cov-2 Infection. Nat Cardiovasc Res 1, 1187–1194 (2022). https://doi.org/10.1038/s44161-022-00177-8
[8] Jung, SW., Jeon, J.J., Kim, Y.H. et al. Long-term risk of autoimmune diseases after mRNA-based SARS-CoV2 vaccination in a Korean, nationwide, population-based cohort study. Nat Commun 15, 6181 (2024). https://doi.org/10.1038/s41467-024-50656-8
[9] Chemaitelly, H., Ayoub, H.H., AlMukdad, S. et al. Duration of mRNA vaccine protection against SARS-CoV-2 Omicron BA.1 and BA.2 subvariants in Qatar. Nat Commun 13, 3082 (2022). https://doi.org/10.1038/s41467-022-30895-3
[10] Nabin K Shrestha, Patrick C Burke, Amy S Nowacki, James F Simon, Amanda Hagen, Steven M Gordon, Effectiveness of the Coronavirus Disease 2019 Bivalent Vaccine, Open Forum Infectious Diseases, Volume 10, Issue 6, June 2023, ofad209, https://doi.org/10.1093/ofid/ofad209
[11] Roltgen et al. Immune imprinting, breadth of variant recognition, and germinal center response in human SARS-CoV-2 infection and vaccination. Cell 185, 1025–1040 March 17, 2022. https://doi.org/10.1016/j.cell.2022.01.018
[12] Brogna C, Cristoni S, Marino G, Montano L, Viduto V, Fabrowski M, Lettieri G, Piscopo M. Detection of recombinant Spike protein in the blood of individuals vaccinated against SARS-CoV-2: Possible molecular mechanisms. Proteomics Clin Appl. 2023 Nov;17(6):e2300048. doi: 10.1002/prca.202300048. Epub 2023 Aug 31. PMID: 37650258.
[13] Yonker L, et al. Circulating Spike Protein Detected in Post-COVID-19 mRNA Vaccine Myocarditis. AHA Journal. January 4, 2023. https://doi.org/10.1161/CIRCULATIONAHA.122.061025
[14] Speicher DJ et al. DNA fragments detected in COVID-19 vaccines in Canada. Oct. 18, 2023. https://osf.io/preprints/osf/mjc97_v1
[15] The Hope Accord. July 3, 2024. https://thehopeaccord.org/
[16] Palmer, M and Gilthorpe, J. COVID-19 mRNA vaccines contain excessive quantities of bacterial DNA: evidence and implications. April 5, 2023. https://doctors4covidethics.org/covid-19-mrna-vaccines-contain-excessive-quantities-of-bacterial-dna-evidence-and-implications/
[17] Palmer, M. Alternate mechanisms of mRNA vaccine toxicity: which one is the main culprit? May 3, 2023. https://doctors4covidethics.org/alternate-mechanisms-of-mrna-vaccine-toxicity-which-one-is-the-main-culprit/
[18] Doctors for COVID Ethics. mRNA Vaccines are Dangerous from First Principles of Immunology. August 24, 2023. https://doctors4covidethics.org/mrna-vaccines-are-dangerous-from-first-principles-of-immunology/
[19] Risch, H. Big Pharma Still Won’t Come Clean About The Covid Shot’s Deadly Side Effects The Federalist. November 26, 2024. https://thefederalist.com/2024/11/26/big-pharma-still-wont-come-clean-about-the-covid-shots-deadly-side-effects/
[20] Myers T, et al. The v-safe after vaccination health checker: Active vaccine safety monitoring during CDC’s COVID-19 pandemic response. Vaccine. Volume 41, Issue 7, 2023, Pages 1310-1318, ISSN 0264-410X, https://doi.org/10.1016/j.vaccine.2022.12.031.
[21] Siri, A. V-Safe Part 7: CDC Deceived the Public With Limited Release of V-Safe Check-the-Box Data Until Forced to Release it All. February 14, 2023.

[22] Siri, A. V-Safe Part 6: A First Look at What the V-Safe Check-the-Box Data Reveals! February 8, 2023. https://aaronsiri.substack.com/p/v-safe-part-6-a-first-look-at-what
[23] https://stacks.cdc.gov/view/cdc/118999
[24] https://www.cdc.gov/nchs/data/vsrr/vsrr031.pdf
[25] https://www.cdc.gov/mmwr/volumes/73/wr/mm7331a1.htm?s_cid=mm7331a1_w
[26] Bridle B, Risch H. Toxic Shot: Facing the Dangers of the COVID “Vaccines”. 2024.
[27] https://fred.stlouisfed.org/series/LNU01074597
[28] https://www.cdc.gov/nchs/nvss/vsrr/covid19/index.htm
[29] https://ec.europa.eu/eurostat/web/products-eurostat-news/w/DDN-20230217-%201
[30] Cuffe, R and Schraer, R. Excess deaths in 2022 among worst in 50 years. BBC News. Jan 10, 2023. https://www.bbc.com/news/health-64209221
[31] Ragnitz, J. 180,000 More People Died Than Normally Expected in Germany during the Covid Years. ifo Institute. Jan. 20, 2023. https://www.ifo.de/en/press-release/2023-01-20/180000-more-people-died-normally-expected-germany-during-covid-years
[32] Dumeau, S. La surmortalité en France a été plus élevée en 2022 que pendant le Covid. June 6, 2023. https://www.lesechos.fr/politique-societe/societe/en-2022-la-surmortalite-en-france-a-ete-plus-elevee-que-pendant-la-pandemie-1949597
[33] Whelan, C. Thousands more Aussies dying as ‘excess deaths’ rise. April 7, 2023. https://www.news.com.au/lifestyle/health/health-problems/thousands-more-aussies-dying-as-excess-deaths-rise/news-story/2e6d46659884d19d9a8d27c52808cf61
[34] Cosentino M, Marino F. Understanding the Pharmacology of COVID-19 mRNA Vaccines: Playing Dice with the Spike? International Journal of Molecular Sciences. 2022; 23(18):10881. https://doi.org/10.3390/ijms231810881
[35] Halma MTJ, Plothe C, Marik P, Lawrie TA. Strategies for the Management of Spike Protein-Related Pathology. Microorganisms. 2023; 11(5):1308. https://doi.org/10.3390/microorganisms11051308
[36] Parry PI, Lefringhausen A, Turni C, Neil CJ, Cosford R, Hudson NJ, Gillespie J. ‘Spikeopathy’: COVID-19 Spike Protein Is Pathogenic, from Both Virus and Vaccine mRNA. Biomedicines. 2023; 11(8):2287. https://doi.org/10.3390/biomedicines11082287
[37] Trougakos, Ioannis P. et al. Adverse effects of COVID-19 mRNA vaccines: the spike hypothesis.Trends in Molecular Medicine, Volume 28, Issue 7, 542 – 554. July 2022. https://www.cell.com/trends/molecular-medicine/fulltext/S1471-4914(22)00103-4
[38] “JW v HHS FDA Pfizer BioNTech Vaccine prod 3 02418 “ March 21, 2022. https://www.judicialwatch.org/documents/jw-v-hhs-fda-pfizer-biontech-vaccine-prod-3-02418/
[39] European Medicines Agency. Assessment Report. Feb. 19, 2021. https://www.ema.europa.eu/en/documents/assessment-report/comirnaty-epar-public-assessment-report_en.pdf
[40] Pfizer Inc. SARS-CoV-2 mRNA Vaccine (BNT162, PF-07302048): 2.6.4 Summary of Pharmacokinetic Studies. Pfizer Confidential; Accessed Feb. 9, 2025. https://www.docdroid.net/xq0Z8B0/pfizer-report-japanese-government-pdf
[41] Castruita, J A C., et al. SARS-CoV-2 spike mRNA vaccine sequences circulate in blood up to 28 days after COVID-19 vaccination. January 17, 2023. https://doi.org/10.1111/apm.13294
[42] Baumeier C, Aleshcheva G, Harms D, Gross U, Hamm C, Assmus B, Westenfeld R, Kelm M, Rammos S, Wenzel P, et al. Intramyocardial Inflammation after COVID-19 Vaccination: An Endomyocardial Biopsy-Proven Case Series. International Journal of Molecular Sciences. 2022; 23(13):6940. https://doi.org/10.3390/ijms23136940
[43] Cosentino M, Marino F. The spike hypothesis in vaccine-induced adverse effects: questions and answers. Trends in Molecular Medicine. Volume 28, Issue 10, p797-799, October 2022. https://www.cell.com/trends/molecular-medicine/fulltext/S1471-4914(22)00189-7
[44] Attorney General of Texas. Attorney General Ken Paxton Sues Pfizer for Misrepresenting COVID-19 Vaccine Efficacy and Conspiring to Censor Public Discourse. November 30, 2023. https://www.texasattorneygeneral.gov/news/releases/attorney-general-ken-paxton-sues-pfizer-misrepresenting-covid-19-vaccine-efficacy-and-conspiring
[45] The NORTH Group, 2024. "Letter to Heads of State Calling for Suspension of mRNA Vaccines."
[46] European Medicines Agency (2023). EMA/451828/2023. https://www.dropbox.com/scl/fi/0tmz0c3ui0te9jq7qwt37/2023-10-18-Letter-to-MEP-Marcel-de-GraaffRequest-for-the-dire.pdf?rlkey=8hgl56ykrxoq7i4y2t11as9ub&e=1&dl=0
[47] Faksova et al. (2024). COVID-19 vaccines and adverse events of special interest: A multinational Global Vaccine Data Network (GVDN) cohort study of 99 million vaccinated individuals. https://www.sciencedirect.com/science/article/pii/S0264410X24001270
[48] Eudravigilance (2024). https://www.adrreports.eu/en/index.html
[49] Schmeling et al. (2023). Batch-dependent safety of the BNT162b2 mRNA COVID-19 vaccine. https://onlinelibrary.wiley.com/doi/10.1111/eci.13998
[50] Manniche et al. (2024). Reports of Batch-Dependent Suspected Adverse Events of the BNT162b2 mRNA COVID-19 Vaccine: Comparison of Results from Denmark and Sweden. Medicina. https://doi.org/10.3390/medicina60081343
[51] Fürst et al. (2024). Batch-dependent safety of COVID-19 vaccines in the Czech Republic and comparison with data from Denmark. https://onlinelibrary.wiley.com/doi/10.1111/eci.14271
[52] Jablonowski & Hooker (2024). Batch-dependent safety of the BNT162b2 mRNA COVID-19 vaccine in the United States. https://publichealthpolicyjournal.com/batch-dependent-safety-of-the-bnt162b2-mrnacovid-19-vaccine-in-the-united-states/
[53] Faksova K, Walsh D, Jiang Y, Griffin J, Phillips A, Gentile A, et al. COVID-19 vaccines and adverse events of special interest: A multinational Global Vaccine Data Network (GVDN) cohort study of 99 million vaccinated individuals. Vaccine. 2024 Apr 2;42(9):2200-2211. doi: 10.1016/j.vaccine.2024.01.100. Epub 2024 Feb 12. PMID: 38350768.
[54] National Academies of Sciences, Engineering and Medicine. Evidence Review of the Adverse Effects of COVID-19 Vaccination and Intramuscular Vaccine Administration. National Academies Press. 2024. http://nap.nationalacademies.org/27746
[55] AAPS. “COVID-19: Is the Death Rate Higher after Vaccination?” April 27, 2024. https://aapsonline.org/covid-19-is-the-death-rate-higher-after-vaccination/
[56] Twenty-Second Statewide Grand Jury of Florida. Final Report of the Twenty-Second Statewide Grand Jury. Nov. 22, 2024. https://acis-api.flcourts.gov/courts/68f021c4-6a44-4735-9a76-5360b2e8af13/cms/case/172e2f34-0a47-41fa-a92f-6fc5ad21b4c9/docketentrydocuments/014d2065-ab2b-40b7-b42e-534adf57e553
[57] Knudsen B, Prasad V. COVID-19 vaccine induced myocarditis in young males: A systematic review. Eur J Clin Invest. 2023 Apr;53(4):e13947. doi: 10.1111/eci.13947. Epub 2023 Jan 3. PMID: 36576362; PMCID: PMC9880674.
[58] Karlstad, et al. SARS-CoV-2 Vaccination and Myocarditis in a Nordic Cohort Study of 23 Million Residents. JAMA Cardiol. 2022 Jun 1;7(6):600-612. doi: 10.1001/jamacardio.2022.0583. PMID: 35442390; PMCID: PMC9021987. https://pmc.ncbi.nlm.nih.gov/articles/PMC9021987/
[59] Buchan SA, et al. Epidemiology of Myocarditis and Pericarditis Following mRNA Vaccination by Vaccine Product, Schedule, and Interdose Interval Among Adolescents and Adults in Ontario, Canada. JAMA Netw Open. 2022 Jun 1;5(6):e2218505. doi: 10.1001/jamanetworkopen.2022.18505. PMID: 35749115; PMCID: PMC9233237. https://pubmed.ncbi.nlm.nih.gov/35749115/
[60] Mevorach D, et al. Myocarditis after BNT162b2 mRNA Vaccine against Covid-19 in Israel. N Engl J Med. 2021 Dec 2;385(23):2140-2149. doi: 10.1056/NEJMoa2109730. Epub 2021 Oct 6. PMID: 34614328; PMCID: PMC8531987. https://pubmed.ncbi.nlm.nih.gov/34614328/
[61] Shimabukuro, T. Vaccine Safety Team, CDC COVID-19 Vaccine Task Force. Updates on myocarditis and pericarditis following Moderna COVID-19 vaccination. Advisory Committee on Immunization Practices. February 4, 2022 https://stacks.cdc.gov/view/cdc/114156/cdc_114156_DS1.pdf
[62] Montgomery J, et al. Myocarditis Following Immunization With mRNA COVID-19 Vaccines in Members of the US Military. JAMA Cardiol. 2021 Oct 1. https://pubmed.ncbi.nlm.nih.gov/34185045/
[63] Fraiman J, Erviti J, Jones M, Greenland S, Whelan P, Kaplan RM, Doshi P. Serious adverse events of special interest following mRNA COVID-19 vaccination in randomized trials in adults. Vaccine. 2022 Sep 22;40(40):5798-5805. doi: 10.1016/j.vaccine.2022.08.036. Epub 2022 Aug 31. PMID: 36055877; PMCID: PMC9428332. https://pmc.ncbi.nlm.nih.gov/articles/PMC9428332/
[64] Kouhpayeh H, Ansari H. Adverse events following COVID-19 vaccination: A systematic review and meta-analysis. Int Immunopharmacol. 2022;109:108906. doi:10.1016/j.intimp.2022.108906 https://pubmed.ncbi.nlm.nih.gov/35671640/
[65] Yang D et al. An overview and single-arm meta-analysis of immune-mediated adverse events following COVID-19 vaccination. Front. Pharmacol., 11 June 2024. https://www.frontiersin.org/journals/pharmacology/articles/10.3389/fphar.2024.1308768/full
[66] Yasmin F et al. Adverse events following COVID-19 mRNA vaccines: A systematic review of cardiovascular complication, thrombosis, and thrombocytopenia. Immunity, Inflammation and Disease. March 17, 2023. https://doi.org/10.1002/iid3.807
[67] Knudsen B, Prasad V. COVID-19 vaccine induced myocarditis in young males: A systematic review. Eur J Clin Invest. 2023;53(4):e13947. doi:10.1111/eci.13947 https://pubmed.ncbi.nlm.nih.gov/36576362/
[68] Lai YH, Chen HY, Chiu HH, Kang YN, Wong SB. Peripheral Nervous System Adverse Events after the Administration of mRNA Vaccines: A Systematic Review and Meta-Analysis of Large-Scale Studies. Vaccines (Basel). 2022;10(12):2174. Published 2022 Dec 17. doi:10.3390/vaccines10122174
[69] Iannou et al. Effectiveness of the 2023-to-2024 XBB.1.5 COVID-19 Vaccines Over Long-Term Follow-up: A Target Trial Emulation. Annals of Internal Medicine. February 4, 2025. https://www.acpjournals.org/doi/10.7326/ANNALS-24-01015
[70] Nakatani E, Morioka H, Kikuchi T, et al. (December 13, 2024) Behavioral and Health Outcomes of mRNA COVID-19 Vaccination: A Case-Control Study in Japanese Small and Medium-Sized Enterprises. Cureus 16(12): e75652. doi:10.7759/cureus.75652
[71] Eythorsson E, Runolfsdottir HL, Ingvarsson RF, Sigurdsson MI, Palsson R. Rate of SARS-CoV-2 Reinfection During an Omicron Wave in Iceland. JAMA Netw Open. 2022;5(8):e2225320. doi:10.1001/jamanetworkopen.2022.25320
[72] Chemaitelly, H., Ayoub, H.H., AlMukdad, S. et al. Duration of mRNA vaccine protection against SARS-CoV-2 Omicron BA.1 and BA.2 subvariants in Qatar. Nat Commun 13, 3082 (2022). https://doi.org/10.1038/s41467-022-30895-3
[73] Nabin K Shrestha, Patrick C Burke, Amy S Nowacki, James F Simon, Amanda Hagen, Steven M Gordon, Effectiveness of the Coronavirus Disease 2019 Bivalent Vaccine, Open Forum Infectious Diseases, Volume 10, Issue 6, June 2023, ofad209, https://doi.org/10.1093/ofid/ofad209
[74] Leora R Feldstein, et al. Protection From COVID-19 Vaccination and Prior SARS-CoV-2 Infection Among Children Aged 6 Months–4 Years, United States, September 2022–April 2023, Journal of the Pediatric Infectious Diseases Society, Volume 14, Issue 1, January 2025, piae121, https://doi.org/10.1093/jpids/piae121
[75] Mead et al,.COVID-19 Modified mRNA “Vaccines”: Lessons Learned from Clinical Trials, Mass Vaccination, and the Bio-Pharmaceutical Complex, Part 2. August 16, 2024. International Journal of Vaccine Theory, Practice, and Research , 3(2), 1275-1344. https://doi.org/10.56098/w66wjg87
[76] Mead et al,. COVID-19 mRNA Vaccines: Lessons Learned from the Registrational Trials and Global Vaccination Campaign. January 2024. https://www.researchgate.net/publication/377667508_COVID-19_mRNA_Vaccines_Lessons_Learned_from_the_Registrational_Trials_and_Global_Vaccination_Campaign
[77] Jewett C. Kennedy sought to stop COVID vaccinations 6 months after rollout. The New York Times. January 17, 2025. https://www.nytimes.com/2025/01/17/health/rfk-jr-covid-vaccines.html
[78] Reed G, Hendlin Y, Desikan A, MacKinney T, Berman E, Goldman GT. The disinformation playbook: how industry manipulates the science-policy process—and how to restore scientific integrity. Glob Health. 2021;10:PMC8651604. doi:10.1186/s12992-021-00761-4.
[79] Thacker P. Covid-19: Researcher blows the whistle on data integrity issues in Pfizer’s vaccine trial. Nov. 2, 2021. BMJ 2021;375:n2635 https://doi.org/10.1136/bmj.n2635
[80] UNITED STATES OF AMERICA ex rel. BROOK JACKSON, Plaintiff, v. VENTAVIA RESEARCH GROUP, LLC; PFIZER, INC.; ICON, PLC, Defendants. CIVIL ACTION NO. 1:21-CV-00008. Decided: August 09, 2024. https://caselaw.findlaw.com/court/us-dis-crt-e-d-tex-bea-div/116482929.html
[81] Universal Health Services, Inc. v. United States ex rel. Escobar, 579 US 176 (2016). https://www.law.cornell.edu/supremecourt/text/15-7
[82] Doyle C. Qui Tam: The False Claims Act and Related Federal Statutes. Congressional Research Service. April 26, 2021. https://crsreports.congress.gov/product/pdf/R/R40785
[83] Hulscher N, Bowden M T., McCullough P A.. Review: Calls for Market Removal of COVID-19 Vaccines Intensify as Risks Far Outweigh Theoretical Benefits. Science, Public Health Policy and the Law. 2025 Jan 28; v6.2019-2025 https://publichealthpolicyjournal.com/review-of-calls-for-market-removal-of-covid-19-vaccines-intensify-risks-far-outweigh-theoretical-benefits/
[i] Jewett C. Kennedy sought to stop COVID vaccinations 6 months after rollout. The New York Times. January 17, 2025. https://www.nytimes.com/2025/01/17/health/rfk-jr-covid-vaccines.html
[ii] Reed G, Hendlin Y, Desikan A, MacKinney T, Berman E, Goldman GT. The disinformation playbook: how industry manipulates the science-policy process—and how to restore scientific integrity. Glob Health. 2021;10:PMC8651604. doi:10.1186/s12992-021-00761-4.
[iii] Thacker P. Covid-19: Researcher blows the whistle on data integrity issues in Pfizer’s vaccine trial. Nov. 2, 2021. BMJ 2021;375:n2635 https://doi.org/10.1136/bmj.n2635
[iv] UNITED STATES OF AMERICA ex rel. BROOK JACKSON, Plaintiff, v. VENTAVIA RESEARCH GROUP, LLC; PFIZER, INC.; ICON, PLC, Defendants. CIVIL ACTION NO. 1:21-CV-00008. Decided: August 09, 2024. https://caselaw.findlaw.com/court/us-dis-crt-e-d-tex-bea-div/116482929.html
[v] Universal Health Services, Inc. v. United States ex rel. Escobar, 579 US 176 (2016). https://www.law.cornell.edu/supremecourt/text/15-7
[vi] Doyle C. Qui Tam: The False Claims Act and Related Federal Statutes. Congressional Research Service. April 26, 2021. https://crsreports.congress.gov/product/pdf/R/R40785
[vii] Hulscher N, Bowden M T., McCullough P A.. Review: Calls for Market Removal of COVID-19 Vaccines Intensify as Risks Far Outweigh Theoretical Benefits. Science, Public Health Policy and the Law. 2025 Jan 28; v6.2019-2025 https://publichealthpolicyjournal.com/review-of-calls-for-market-removal-of-covid-19-vaccines-intensify-risks-far-outweigh-theoretical-benefits/
[i] Fraiman J, Erviti J, Jones M, Greenland S, Whelan P, Kaplan RM, Doshi P. Serious adverse events of special interest following mRNA COVID-19 vaccination in randomized trials in adults. Vaccine. 2022 Sep 22;40(40):5798-5805. doi: 10.1016/j.vaccine.2022.08.036. Epub 2022 Aug 31. PMID: 36055877; PMCID: PMC9428332. https://pmc.ncbi.nlm.nih.gov/articles/PMC9428332/
[ii] Kouhpayeh H, Ansari H. Adverse events following COVID-19 vaccination: A systematic review and meta-analysis. Int Immunopharmacol. 2022;109:108906. doi:10.1016/j.intimp.2022.108906 https://pubmed.ncbi.nlm.nih.gov/35671640/
[iii] Yang D et al. An overview and single-arm meta-analysis of immune-mediated adverse events following COVID-19 vaccination. Front. Pharmacol., 11 June 2024. https://www.frontiersin.org/journals/pharmacology/articles/10.3389/fphar.2024.1308768/full
[iv] Yasmin F et al. Adverse events following COVID-19 mRNA vaccines: A systematic review of cardiovascular complication, thrombosis, and thrombocytopenia. Immunity, Inflammation and Disease. March 17, 2023. https://doi.org/10.1002/iid3.807
[v] Knudsen B, Prasad V. COVID-19 vaccine induced myocarditis in young males: A systematic review. Eur J Clin Invest. 2023;53(4):e13947. doi:10.1111/eci.13947 https://pubmed.ncbi.nlm.nih.gov/36576362/
[vi] Lai YH, Chen HY, Chiu HH, Kang YN, Wong SB. Peripheral Nervous System Adverse Events after the Administration of mRNA Vaccines: A Systematic Review and Meta-Analysis of Large-Scale Studies. Vaccines (Basel). 2022;10(12):2174. Published 2022 Dec 17. doi:10.3390/vaccines10122174
[vii] Iannou et al. Effectiveness of the 2023-to-2024 XBB.1.5 COVID-19 Vaccines Over Long-Term Follow-up: A Target Trial Emulation. Annals of Internal Medicine. February 4, 2025. https://www.acpjournals.org/doi/10.7326/ANNALS-24-01015
[viii] Nakatani E, Morioka H, Kikuchi T, et al. (December 13, 2024) Behavioral and Health Outcomes of mRNA COVID-19 Vaccination: A Case-Control Study in Japanese Small and Medium-Sized Enterprises. Cureus 16(12): e75652. doi:10.7759/cureus.75652
[ix] Eythorsson E, Runolfsdottir HL, Ingvarsson RF, Sigurdsson MI, Palsson R. Rate of SARS-CoV-2 Reinfection During an Omicron Wave in Iceland. JAMA Netw Open. 2022;5(8):e2225320. doi:10.1001/jamanetworkopen.2022.25320
[x][x] Chemaitelly, H., Ayoub, H.H., AlMukdad, S. et al. Duration of mRNA vaccine protection against SARS-CoV-2 Omicron BA.1 and BA.2 subvariants in Qatar. Nat Commun 13, 3082 (2022). https://doi.org/10.1038/s41467-022-30895-3
[xi] Nabin K Shrestha, Patrick C Burke, Amy S Nowacki, James F Simon, Amanda Hagen, Steven M Gordon, Effectiveness of the Coronavirus Disease 2019 Bivalent Vaccine, Open Forum Infectious Diseases, Volume 10, Issue 6, June 2023, ofad209, https://doi.org/10.1093/ofid/ofad209
[xii] Leora R Feldstein, et al. Protection From COVID-19 Vaccination and Prior SARS-CoV-2 Infection Among Children Aged 6 Months–4 Years, United States, September 2022–April 2023, Journal of the Pediatric Infectious Diseases Society, Volume 14, Issue 1, January 2025, piae121, https://doi.org/10.1093/jpids/piae121
[xiii] Mead et al,.COVID-19 Modified mRNA “Vaccines”: Lessons Learned from Clinical Trials, Mass Vaccination, and the Bio-Pharmaceutical Complex, Part 2. August 16, 2024. International Journal of Vaccine Theory, Practice, and Research , 3(2), 1275-1344. https://doi.org/10.56098/w66wjg87
[xiv] Mead et al,. COVID-19 mRNA Vaccines: Lessons Learned from the Registrational Trials and Global Vaccination Campaign. January 2024. https://www.researchgate.net/publication/377667508_COVID-19_mRNA_Vaccines_Lessons_Learned_from_the_Registrational_Trials_and_Global_Vaccination_Campaign
[i] Twenty-Second Statewide Grand Jury of Florida. Final Report of the Twenty-Second Statewide Grand Jury. Nov. 22, 2024. https://acis-api.flcourts.gov/courts/68f021c4-6a44-4735-9a76-5360b2e8af13/cms/case/172e2f34-0a47-41fa-a92f-6fc5ad21b4c9/docketentrydocuments/014d2065-ab2b-40b7-b42e-534adf57e553
[ii] Knudsen B, Prasad V. COVID-19 vaccine induced myocarditis in young males: A systematic review. Eur J Clin Invest. 2023 Apr;53(4):e13947. doi: 10.1111/eci.13947. Epub 2023 Jan 3. PMID: 36576362; PMCID: PMC9880674.
[iii] Karlstad, et al. SARS-CoV-2 Vaccination and Myocarditis in a Nordic Cohort Study of 23 Million Residents. JAMA Cardiol. 2022 Jun 1;7(6):600-612. doi: 10.1001/jamacardio.2022.0583. PMID: 35442390; PMCID: PMC9021987. https://pmc.ncbi.nlm.nih.gov/articles/PMC9021987/
[iv] Buchan SA, et al. Epidemiology of Myocarditis and Pericarditis Following mRNA Vaccination by Vaccine Product, Schedule, and Interdose Interval Among Adolescents and Adults in Ontario, Canada. JAMA Netw Open. 2022 Jun 1;5(6):e2218505. doi: 10.1001/jamanetworkopen.2022.18505. PMID: 35749115; PMCID: PMC9233237. https://pubmed.ncbi.nlm.nih.gov/35749115/
[v] Mevorach D, et al. Myocarditis after BNT162b2 mRNA Vaccine against Covid-19 in Israel. N Engl J Med. 2021 Dec 2;385(23):2140-2149. doi: 10.1056/NEJMoa2109730. Epub 2021 Oct 6. PMID: 34614328; PMCID: PMC8531987. https://pubmed.ncbi.nlm.nih.gov/34614328/
[vi] Shimabukuro, T. Vaccine Safety Team, CDC COVID-19 Vaccine Task Force. Updates on myocarditis and pericarditis following Moderna COVID-19 vaccination. Advisory Committee on Immunization Practices. February 4, 2022 https://stacks.cdc.gov/view/cdc/114156/cdc_114156_DS1.pdf
[vii] Montgomery J, et al. Myocarditis Following Immunization With mRNA COVID-19 Vaccines in Members of the US Military. JAMA Cardiol. 2021 Oct 1. https://pubmed.ncbi.nlm.nih.gov/34185045/
[i] Florida Department of Health. Florida State Surgeon General Calls for Halt in the Use of COVID-19 mRNA Vaccines. Jan. 03, 2024. https://www.floridahealth.gov/newsroom/2024/01/20240103-halt-use-covid19-mrna-vaccines.pr.html
[ii] Florida Department of Health. Updated Guidance for COVID-19 Boosters for the Fall and Winter 2024–2025 Season. Sept. 12, 2024. https://www.floridahealth.gov/newsroom/2024/09/20210912-UpdatedGuidanceCOVID-19.html
[iii] Buergin N, Lopez-Ayala P, et al. Sex-specific differences in myocardial injury incidence after COVID-19 mRNA-1273 booster vaccination. European Journal of Heart Failure. July 20, 2023. https://onlinelibrary.wiley.com/doi/10.1002/ejhf.2978
[iv] Mansanguan S, Charunwatthana P, Piyaphanee W, Dechkhajorn W, Poolcharoen A, Mansanguan C. Cardiovascular Manifestation of the BNT162b2 mRNA COVID-19 Vaccine in Adolescents. Tropical Medicine and Infectious Disease. 2022; 7(8):196. https://doi.org/10.3390/tropicalmed7080196
[v] Kwan, A.C., Ebinger, J.E., Wei, J. et al. Apparent risks of postural orthostatic tachycardia syndrome diagnoses after COVID-19 vaccination and SARS-Cov-2 Infection. Nat Cardiovasc Res 1, 1187–1194 (2022). https://doi.org/10.1038/s44161-022-00177-8
[vi] Jung, SW., Jeon, J.J., Kim, Y.H. et al. Long-term risk of autoimmune diseases after mRNA-based SARS-CoV2 vaccination in a Korean, nationwide, population-based cohort study. Nat Commun 15, 6181 (2024). https://doi.org/10.1038/s41467-024-50656-8
[vii] Chemaitelly, H., Ayoub, H.H., AlMukdad, S. et al. Duration of mRNA vaccine protection against SARS-CoV-2 Omicron BA.1 and BA.2 subvariants in Qatar. Nat Commun 13, 3082 (2022). https://doi.org/10.1038/s41467-022-30895-3
[viii] Nabin K Shrestha, Patrick C Burke, Amy S Nowacki, James F Simon, Amanda Hagen, Steven M Gordon, Effectiveness of the Coronavirus Disease 2019 Bivalent Vaccine, Open Forum Infectious Diseases, Volume 10, Issue 6, June 2023, ofad209, https://doi.org/10.1093/ofid/ofad209
[ix] Roltgen et al. Immune imprinting, breadth of variant recognition, and germinal center response in human SARS-CoV-2 infection and vaccination. Cell 185, 1025–1040 March 17, 2022. https://doi.org/10.1016/j.cell.2022.01.018
[x] Brogna C, Cristoni S, Marino G, Montano L, Viduto V, Fabrowski M, Lettieri G, Piscopo M. Detection of recombinant Spike protein in the blood of individuals vaccinated against SARS-CoV-2: Possible molecular mechanisms. Proteomics Clin Appl. 2023 Nov;17(6):e2300048. doi: 10.1002/prca.202300048. Epub 2023 Aug 31. PMID: 37650258.
[xi] Yonker L, et al. Circulating Spike Protein Detected in Post-COVID-19 mRNA Vaccine Myocarditis. AHA Journal. January 4, 2023. https://doi.org/10.1161/CIRCULATIONAHA.122.061025
[xii] Speicher DJ et al. DNA fragments detected in COVID-19 vaccines in Canada. Oct. 18, 2023. https://osf.io/preprints/osf/mjc97_v1
[xiii] The Hope Accord. July 3, 2024. https://thehopeaccord.org/
[xiv] Palmer, M and Gilthorpe, J. COVID-19 mRNA vaccines contain excessive quantities of bacterial DNA: evidence and implications. April 5, 2023. https://doctors4covidethics.org/covid-19-mrna-vaccines-contain-excessive-quantities-of-bacterial-dna-evidence-and-implications/
[xv] Palmer, M. Alternate mechanisms of mRNA vaccine toxicity: which one is the main culprit? May 3, 2023. https://doctors4covidethics.org/alternate-mechanisms-of-mrna-vaccine-toxicity-which-one-is-the-main-culprit/
[xvi] Doctors for COVID Ethics. mRNA Vaccines are Dangerous from First Principles of Immunology. August 24, 2023. https://doctors4covidethics.org/mrna-vaccines-are-dangerous-from-first-principles-of-immunology/
[xvii] Risch, H. Big Pharma Still Won’t Come Clean About The Covid Shot’s Deadly Side Effects The Federalist. November 26, 2024. https://thefederalist.com/2024/11/26/big-pharma-still-wont-come-clean-about-the-covid-shots-deadly-side-effects/
[xviii] Myers T, et al. The v-safe after vaccination health checker: Active vaccine safety monitoring during CDC’s COVID-19 pandemic response. Vaccine. Volume 41, Issue 7, 2023, Pages 1310-1318, ISSN 0264-410X, https://doi.org/10.1016/j.vaccine.2022.12.031.
[xix] Siri, A. V-Safe Part 7: CDC Deceived the Public With Limited Release of V-Safe Check-the-Box Data Until Forced to Release it All. February 14, 2023.
[xx] Siri, A. V-Safe Part 6: A First Look at What the V-Safe Check-the-Box Data Reveals! February 8, 2023. https://aaronsiri.substack.com/p/v-safe-part-6-a-first-look-at-what
[xxi] https://stacks.cdc.gov/view/cdc/118999
[xxii] https://www.cdc.gov/nchs/data/vsrr/vsrr031.pdf
[xxiii] https://www.cdc.gov/mmwr/volumes/73/wr/mm7331a1.htm?s_cid=mm7331a1_w
[xxiv] Bridle B, Risch H. Toxic Shot: Facing the Dangers of the COVID “Vaccines”. 2024.
[xxv] https://fred.stlouisfed.org/series/LNU01074597
[xxvi] https://www.cdc.gov/nchs/nvss/vsrr/covid19/index.htm
[xxvii] https://ec.europa.eu/eurostat/web/products-eurostat-news/w/DDN-20230217-%201
[xxviii] Cuffe, R and Schraer, R. Excess deaths in 2022 among worst in 50 years. BBC News. Jan 10, 2023. https://www.bbc.com/news/health-64209221
[xxix] Ragnitz, J. 180,000 More People Died Than Normally Expected in Germany during the Covid Years. ifo Institute. Jan. 20, 2023. https://www.ifo.de/en/press-release/2023-01-20/180000-more-people-died-normally-expected-germany-during-covid-years
[xxx] Dumeau, S. La surmortalité en France a été plus élevée en 2022 que pendant le Covid. June 6, 2023. https://www.lesechos.fr/politique-societe/societe/en-2022-la-surmortalite-en-france-a-ete-plus-elevee-que-pendant-la-pandemie-1949597
[xxxi] Whelan, C. Thousands more Aussies dying as ‘excess deaths’ rise. April 7, 2023. https://www.news.com.au/lifestyle/health/health-problems/thousands-more-aussies-dying-as-excess-deaths-rise/news-story/2e6d46659884d19d9a8d27c52808cf61
[xxxii] Cosentino M, Marino F. Understanding the Pharmacology of COVID-19 mRNA Vaccines: Playing Dice with the Spike? International Journal of Molecular Sciences. 2022; 23(18):10881. https://doi.org/10.3390/ijms231810881
[xxxiii] Halma MTJ, Plothe C, Marik P, Lawrie TA. Strategies for the Management of Spike Protein-Related Pathology. Microorganisms. 2023; 11(5):1308. https://doi.org/10.3390/microorganisms11051308
[xxxiv] Parry PI, Lefringhausen A, Turni C, Neil CJ, Cosford R, Hudson NJ, Gillespie J. ‘Spikeopathy’: COVID-19 Spike Protein Is Pathogenic, from Both Virus and Vaccine mRNA. Biomedicines. 2023; 11(8):2287. https://doi.org/10.3390/biomedicines11082287
[xxxv] Trougakos, Ioannis P. et al. Adverse effects of COVID-19 mRNA vaccines: the spike hypothesis.Trends in Molecular Medicine, Volume 28, Issue 7, 542 – 554. July 2022. https://www.cell.com/trends/molecular-medicine/fulltext/S1471-4914(22)00103-4
[xxxvi] “JW v HHS FDA Pfizer BioNTech Vaccine prod 3 02418 “ March 21, 2022. https://www.judicialwatch.org/documents/jw-v-hhs-fda-pfizer-biontech-vaccine-prod-3-02418/
[xxxvii] European Medicines Agency. Assessment Report. Feb. 19, 2021. https://www.ema.europa.eu/en/documents/assessment-report/comirnaty-epar-public-assessment-report_en.pdf
[xxxviii] Pfizer Inc. SARS-CoV-2 mRNA Vaccine (BNT162, PF-07302048): 2.6.4 Summary of Pharmacokinetic Studies. Pfizer Confidential; Accessed Feb. 9, 2025. https://www.docdroid.net/xq0Z8B0/pfizer-report-japanese-government-pdf
[xxxix] Castruita, J A C., et al. SARS-CoV-2 spike mRNA vaccine sequences circulate in blood up to 28 days after COVID-19 vaccination. January 17, 2023. https://doi.org/10.1111/apm.13294
[xl] Baumeier C, Aleshcheva G, Harms D, Gross U, Hamm C, Assmus B, Westenfeld R, Kelm M, Rammos S, Wenzel P, et al. Intramyocardial Inflammation after COVID-19 Vaccination: An Endomyocardial Biopsy-Proven Case Series. International Journal of Molecular Sciences. 2022; 23(13):6940. https://doi.org/10.3390/ijms23136940
[xli] Cosentino M, Marino F. The spike hypothesis in vaccine-induced adverse effects: questions and answers. Trends in Molecular Medicine. Volume 28, Issue 10, p797-799, October 2022. https://www.cell.com/trends/molecular-medicine/fulltext/S1471-4914(22)00189-7
[xlii] Attorney General of Texas. Attorney General Ken Paxton Sues Pfizer for Misrepresenting COVID-19 Vaccine Efficacy and Conspiring to Censor Public Discourse. November 30, 2023. https://www.texasattorneygeneral.gov/news/releases/attorney-general-ken-paxton-sues-pfizer-misrepresenting-covid-19-vaccine-efficacy-and-conspiring
[xliii] The NORTH Group, 2024. "Letter to Heads of State Calling for Suspension of mRNA Vaccines."
[xliv] European Medicines Agency (2023). EMA/451828/2023. https://www.dropbox.com/scl/fi/0tmz0c3ui0te9jq7qwt37/2023-10-18-Letter-to-MEP-Marcel-de-GraaffRequest-for-the-dire.pdf?rlkey=8hgl56ykrxoq7i4y2t11as9ub&e=1&dl=0
[xlv] Faksova et al. (2024). COVID-19 vaccines and adverse events of special interest: A multinational Global Vaccine Data Network (GVDN) cohort study of 99 million vaccinated individuals. https://www.sciencedirect.com/science/article/pii/S0264410X24001270
[xlvi] Eudravigilance (2024). https://www.adrreports.eu/en/index.html
[xlvii] Schmeling et al. (2023). Batch-dependent safety of the BNT162b2 mRNA COVID-19 vaccine. https://onlinelibrary.wiley.com/doi/10.1111/eci.13998
[xlviii] Manniche et al. (2024). Reports of Batch-Dependent Suspected Adverse Events of the BNT162b2 mRNA COVID-19 Vaccine: Comparison of Results from Denmark and Sweden. Medicina. https://doi.org/10.3390/medicina60081343
[xlix] Fürst et al. (2024). Batch-dependent safety of COVID-19 vaccines in the Czech Republic and comparison with data from Denmark. https://onlinelibrary.wiley.com/doi/10.1111/eci.14271
[l] Jablonowski & Hooker (2024). Batch-dependent safety of the BNT162b2 mRNA COVID-19 vaccine in the United States. https://publichealthpolicyjournal.com/batch-dependent-safety-of-the-bnt162b2-mrnacovid-19-vaccine-in-the-united-states/
[li] Faksova K, Walsh D, Jiang Y, Griffin J, Phillips A, Gentile A, et al. COVID-19 vaccines and adverse events of special interest: A multinational Global Vaccine Data Network (GVDN) cohort study of 99 million vaccinated individuals. Vaccine. 2024 Apr 2;42(9):2200-2211. doi: 10.1016/j.vaccine.2024.01.100. Epub 2024 Feb 12. PMID: 38350768.
[lii] National Academies of Sciences, Engineering and Medicine. Evidence Review of the Adverse Effects of COVID-19 Vaccination and Intramuscular Vaccine Administration. National Academies Press. 2024. http://nap.nationalacademies.org/27746
[liii] AAPS. “COVID-19: Is the Death Rate Higher after Vaccination?” April 27, 2024. https://aapsonline.org/covid-19-is-the-death-rate-higher-after-vaccination/
[i] Shibata H, Nomura Y, Kawakami T, Yamamoto E, Ando D, Uchiyama N, Tokumoto H, Koide T, Sakoda H, Yoshida H, Abe Y, Hakamatsuka T, Ikarashi Y, Haishima Y, Ishii-Watabe A, Izutsu KI, Honma M, Goda Y. [Investigation of Foreign Particles in Moderna COVID-19 Vaccine]. Yakugaku Zasshi. 2022;142(8):867-874. Japanese. doi: 10.1248/yakushi.22-00067. PMID: 35908947.
[ii] Wingrove P. Exclusive: US FDA finds control lapses at Moderna manufacturing plant. Reuters. December 15, 2023. https://www.reuters.com/business/healthcare-pharmaceuticals/us-fda-finds-control-lapses-moderna-manufacturing-plant-2023-12-15